WO2012099258A1 - 脱毛症治療剤 - Google Patents
脱毛症治療剤 Download PDFInfo
- Publication number
- WO2012099258A1 WO2012099258A1 PCT/JP2012/051272 JP2012051272W WO2012099258A1 WO 2012099258 A1 WO2012099258 A1 WO 2012099258A1 JP 2012051272 W JP2012051272 W JP 2012051272W WO 2012099258 A1 WO2012099258 A1 WO 2012099258A1
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- alopecia
- cnp
- bnp
- hair
- subject
- Prior art date
Links
Images
































































Classifications
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K38/00—Medicinal preparations containing peptides
- A61K38/16—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof
- A61K38/17—Peptides having more than 20 amino acids; Gastrins; Somatostatins; Melanotropins; Derivatives thereof from animals; from humans
- A61K38/22—Hormones
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/13—Amines
- A61K31/14—Quaternary ammonium compounds, e.g. edrophonium, choline
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/33—Heterocyclic compounds
- A61K31/395—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins
- A61K31/495—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins having six-membered rings with two or more nitrogen atoms as the only ring heteroatoms, e.g. piperazine or tetrazines
- A61K31/505—Pyrimidines; Hydrogenated pyrimidines, e.g. trimethoprim
- A61K31/506—Pyrimidines; Hydrogenated pyrimidines, e.g. trimethoprim not condensed and containing further heterocyclic rings
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/56—Compounds containing cyclopenta[a]hydrophenanthrene ring systems; Derivatives thereof, e.g. steroids
- A61K31/57—Compounds containing cyclopenta[a]hydrophenanthrene ring systems; Derivatives thereof, e.g. steroids substituted in position 17 beta by a chain of two carbon atoms, e.g. pregnane or progesterone
- A61K31/573—Compounds containing cyclopenta[a]hydrophenanthrene ring systems; Derivatives thereof, e.g. steroids substituted in position 17 beta by a chain of two carbon atoms, e.g. pregnane or progesterone substituted in position 21, e.g. cortisone, dexamethasone, prednisone or aldosterone
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/70—Carbohydrates; Sugars; Derivatives thereof
- A61K31/7028—Compounds having saccharide radicals attached to non-saccharide compounds by glycosidic linkages
- A61K31/7034—Compounds having saccharide radicals attached to non-saccharide compounds by glycosidic linkages attached to a carbocyclic compound, e.g. phloridzin
- A61K31/7036—Compounds having saccharide radicals attached to non-saccharide compounds by glycosidic linkages attached to a carbocyclic compound, e.g. phloridzin having at least one amino group directly attached to the carbocyclic ring, e.g. streptomycin, gentamycin, amikacin, validamycin, fortimicins
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K45/00—Medicinal preparations containing active ingredients not provided for in groups A61K31/00 - A61K41/00
- A61K45/06—Mixtures of active ingredients without chemical characterisation, e.g. antiphlogistics and cardiaca
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K8/00—Cosmetics or similar toiletry preparations
- A61K8/18—Cosmetics or similar toiletry preparations characterised by the composition
- A61K8/30—Cosmetics or similar toiletry preparations characterised by the composition containing organic compounds
- A61K8/64—Proteins; Peptides; Derivatives or degradation products thereof
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K9/00—Medicinal preparations characterised by special physical form
- A61K9/0012—Galenical forms characterised by the site of application
- A61K9/0014—Skin, i.e. galenical aspects of topical compositions
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P17/00—Drugs for dermatological disorders
- A61P17/14—Drugs for dermatological disorders for baldness or alopecia
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P37/00—Drugs for immunological or allergic disorders
- A61P37/08—Antiallergic agents
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61Q—SPECIFIC USE OF COSMETICS OR SIMILAR TOILETRY PREPARATIONS
- A61Q7/00—Preparations for affecting hair growth
Definitions
- the present invention relates to A-type natriuretic peptide (ANP), B-type natriuretic peptide (BNP), C-type natriuretic peptide (CNP), derivatives of these natriuretic peptides (NP), and these NPs.
- Alopecia, dandruff, gray hair and seborrheic scalp comprising the above NP chimeric peptides or derivatives of these NP chimeric peptides (hereinafter collectively referred to as “natriuretic peptide (NP)”) as active ingredients It relates to a therapeutic agent and / or a preventive agent.
- the present invention relates to a therapeutic agent for alopecia, dandruff, gray hair, and seborrheic scalp comprising, as an active ingredient, BNP, CNP, a derivative of BNP, a derivative of CNP, a chimeric peptide of CNP or BNP, or a derivative thereof, and / or It relates to preventive agents.
- a therapeutic agent for alopecia, dandruff, gray hair, and seborrheic scalp comprising, as an active ingredient, BNP, CNP, a derivative of BNP, a derivative of CNP, a chimeric peptide of CNP or BNP, or a derivative thereof, and / or It relates to preventive agents.
- the therapeutic agent and / or the preventive agent are simply referred to as a therapeutic agent.
- Alopecia is a disease in which body hair decreases. Hair loss in alopecia can occur anywhere in the whole body, not just the hair. Many of them are not related to life and death, but since they are accompanied by serious mental pain due to their appearance problems, an excellent preventive and therapeutic agent for alopecia is desired. In addition, since alopecia often involves fading of hair color, preventive and therapeutic agents for hair fading associated with alopecia are desired. Furthermore, since alopecia often involves deterioration of the hair quality such as thinning of the hair or shortening of the hair, a preventive and therapeutic agent for the deterioration of hair quality associated with alopecia is desired.
- alopecia are ata, male pattern alopecia, postpartum alopecia, female pattern alopecia, seborrheic alopecia, critical alopecia, senile alopecia, cancer chemotherapeutic alopecia , Alopecia due to radiation exposure, hair loss (Trichotiromania), postmenopausal alopecia, etc.
- alopecias are based on different causes even though the symptoms of hair loss are the same, so the treatment methods are also different.
- androgenetic alopecia based on the action of androgen and alopecia areata suspected of being an immune disease are very different diseases.
- postpartum alopecia, female pattern alopecia, seborrheic alopecia, critical alopecia, senile alopecia, cancer chemotherapeutic alopecia, alopecia due to radiation exposure are based on different causes It is thought that there is no effective treatment.
- Alopecia areata is a coin-sized circle with a clear, patchy hairline that often suddenly occurs without subjective symptoms or prodromal symptoms, and if it does not heal spontaneously, then the range gradually expands and is intractable. It is sexual alopecia. Alopecia areata is suspected of being an autoimmune disease, but the cause is not yet known, and the decisive treatment method is not known.
- Alopecia areata is an autoimmune disease such as thyroid disease represented by Hashimoto's disease, vitiligo vulgaris, systemic lupus erythematosus, indirect rheumatism, myasthenia gravis, bronchial asthma, atopic dermatitis, allergic rhinitis, etc. It is known that it may be associated with other atopic diseases.
- Male pattern alopecia is alopecia due to the effect of male hormones acting on androgen-sensitive hair follicles to soften hair, and affects about half of men and 10-20% of women. It is thought that genetic predisposition is greatly concerned, and in male androgenetic alopecia, the hair on the frontal region and the top of the head becomes soft and thin and eventually the hairline of the forehead recedes and the hair on the top of the head I lose my hair. On the other hand, in female androgenetic alopecia, it is common that the hairline of the entire head becomes thin, centering on the parietal region and the frontal region, without changing the hairline. In male androgenetic alopecia, finasteride cannot be used for female androgenetic alopecia because only about a quarter of patients improve with finasteride and it is contraindicated to administer finasteride to women. .
- Postpartum alopecia is alopecia in which hair that has maintained its growth phase due to estrogen enters a rest period at a stretch by parturition and hair loss increases. Hair loss in postpartum alopecia usually starts around 2 months after birth and lasts until about 6 months after birth, but usually returns within 1 year unless it is an elderly birth, so in most cases no special treatment is required However, hair may not recover naturally.
- Female pattern alopecia is alopecia that is thought to be caused by a decrease in the amount of female hormone estrogen relative to the amount of androgens in the bloodstream. It often develops after menopause, in which case it is also called postmenopausal alopecia. Female pattern alopecia may be ameliorated by hormone replacement therapy, but is often refractory.
- Seborrheic alopecia is alopecia caused by excessive secretion of sebum to the scalp, which causes pores and roots to become inflamed by closing the pores, resulting in hair loss. Seborrheic alopecia improves to some extent by removing sebum by washing the hair, but it is likely to recur and is intractable.
- Critical alopecia is alopecia caused by dandruff closing pores and causing inflammation.
- Critical alopecia is often caused by excessive shampooing, and although it can be relieved by reducing the number of shampooing times or using a shampoo with weak cleaning power, it tends to recur and is refractory.
- Hair loss (Trichotiromania) is alopecia caused by hair loss. Hair loss is a symptom that arises as a result of morbid anxiety and can be treated with behavioral or psychotherapy.
- Senile alopecia is alopecia in which the whole body hair, including the entire hair, gradually becomes thinner with aging regardless of gender differences. It is considered as a natural phenomenon that appears in many people due to aging, and is not currently targeted for treatment. However, as life expectancy increases, societal demands to improve the quality of life for the elderly are increasing, and improvements are required.
- Cancer chemotherapeutic alopecia is alopecia as a side effect of anticancer treatment with cancer chemotherapeutic agents.
- the shock of a patient who loses not only the hair but also the body hair of every part, such as eyebrows, eyelids, nose hair, armpit hair, and pubic hair, is great even if given prior explanation. Therefore, it is a hindrance to the implementation of cancer chemotherapy, so the need for treatment is high.
- alopecia associated with radiation exposure is also alopecia that occurs based on the same mechanism as cancer chemotherapeutic alopecia in that it selectively kills cancer cells by impairing cell division. . Therefore, any drug capable of treating alopecia associated with cancer chemotherapy can also treat alopecia associated with radiation exposure.
- alopecia due to drug side effects such as antithyroid, anticoagulant, thallium, psychotropic agent, ⁇ -blocker, alopecia due to fungi, hair loss due to endocrine abnormalities such as hypopituitarism, hypothyroidism or enhancement Dystrophy, nutritional disorders, hypoalbuminemia, cachexia, iron deficiency anemia, zinc deficiency, homocystinuria, alopecia due to metabolic disorders such as cirrhosis, toxic alopecia, high fever, labor, major surgery, rapid weight Loss and alopecia due to serious illness are known, but these can be dealt with by removing the respective causes.
- female pattern alopecia, seborrheic alopecia and critical alopecia can be dealt with to some extent by removing their respective causes, but are likely to recur and are refractory.
- the cause of female pattern alopecia is thought to be hormonal balance, indications for hormone replacement therapy are menopause, osteoporosis and hyperlipidemia, and female pattern alopecia is not indicated. Since there is a risk of carcinogenesis caused by hormone replacement therapy, hormone replacement therapy is not performed for the purpose of treating female pattern alopecia. Male pattern baldness has not yet been adequately treated, and alopecia areata has little known cause.
- alopecia that is difficult to treat among alopecia is alopecia areata and male pattern alopecia.
- Drugs that can be used to treat androgenetic alopecia include vasodilators such as minoxidil, carpronium chloride and various extracts, androgen activity inhibitors such as finasteride, female hormones such as estrogen, estradiol, and progesterone, antifungal
- vasodilators such as minoxidil, carpronium chloride and various extracts
- androgen activity inhibitors such as finasteride
- female hormones such as estrogen, estradiol, and progesterone
- antifungal There are drugs such as ketoconazole, pentadecane, cytopurine (6-benzylaminopurine), t-flavanone, and adenosine.
- “Dermatological treatment guidelines for male pattern alopecia 2010” by the Japanese Dermatological Association recommends that the above-mentioned drugs have a recommendation level A (strongly recommended to do), a recommendation level B (recommended to do), a recommendation level Evaluation is based on five levels: C1 (you may consider doing it, but there is no sufficient basis), recommendation level C2 (not recommended because there is no basis), and recommendation level D (recommended not to do) .
- a treatment method of recommendation degree A minoxidil, a vasodilator, and finasteride, a testosterone 5 ⁇ -reductase inhibitor, are mentioned.
- Minoxidil topical solution for male cases “5% minoxidil topical solution for male cases “1% Minoxidil topical solution should be used as a first-line treatment for female cases and for female cases”, and “Finasteride” should be used as a first-line treatment for male cases. On the other hand, it should not be used for female cases. " On the other hand, the guideline categorizes the C1 recommendations for carpronium chloride, pentadecane, cytopurine, t-flavanone, adenosine and ketoconazole as “you may consider doing it but there is no good basis”. About cephalanthin, the recommendation sentence “It is better not to use” is attached, and it is classified into the recommendation degree of C2.
- minoxidil has side effects such as drug-induced contact alopecia, hair hyperplasia, blood pressure lowering, heart rate reduction, etc., and there is a problem that the symptoms relapse immediately after stopping use.
- Female hormone drugs are at risk of thrombosis.
- finasteride has side effects such as prostate hyperplasia, erectile dysfunction, and ejaculation disorders, and symptoms relapse after use and are contraindicated in pregnant women.
- Non-patent Document 3 the clinical effect of finasteride was confirmed based on the photographic evaluation of the parietal region. That is, although the hair thickening effect of finasteride at the parietal region or O-type site of male pattern alopecia has been confirmed, there is no known evidence of the hair growth effect on hair loss at the frontal region or M-type site. Therefore, for male pattern alopecia, it shows a clear therapeutic effect, persists for a certain period even if it is discontinued, shows clear efficacy against hair loss other than the top of the head, and has fewer side effects. Treatment is needed.
- Alopecia areata is the most common disease of acquired alopecia and occurs in 0.1 to 0.2% of the population in the United States, which seems similar in Japan It is. Alopecia areata can be affected at any age. A quarter of alopecia areata develops before the age of 15 and is alopecia relatively common in children. Severe alopecia areata is also common in children, such as all head and whole body. There is no gender difference in alopecia areata. About one-quarter of patients with alopecia areata have characteristic symptom changes such as small dents and lateral grooves.
- alopecia areata is basically refractory as the hair loss area is larger, severity classification based on the hair loss area has also been considered (Non-patent Document 4).
- Patients with alopecia areata have many physical problems other than hair loss, but the patient suffers deeply, and mental damage and QOL decrease are large. Therefore, not treated with any method but is positioned as skin diseases should not, effective treatment method at present, little.
- alopecia The clinical classification of alopecia areata depends on the number, extent and form of alopecia, [1]. Normal alopecia areata Single type: A single bald area is observed Multiple type: Multiple bald areas are recognized [2]. Total head alopecia: A bald patch spread to the entire head [3]. Generalized alopecia: Alopecia that spreads throughout the body [4]. Serpentine alopecia: Classified as a band with hairline hair loss.
- the alopecia areata evaluation guideline in the United States determines the severity based on the ratio of the hair loss area to the total area of the head (S) and the degree of hair loss other than the head (B). is doing.
- S0 No hair loss is observed.
- S1 Less than 25% of hair loss nest
- S2 25-49% of loss of hair
- S3 50% to 74% hair loss nest
- S4 75 to 99% of hair loss nest
- S5 100% hair loss
- B0 No hair loss other than the head
- B1 Partial hair loss other than the head is observed
- B2 It is defined as hair loss of the whole body, and alopecia areata is more severe as the range of hair loss is wider It is incurable.
- Non-patent Document 5 The etiology of alopecia areata is recently considered to be an autoimmune disease against hair follicle tissue.
- Non-patent Document 6 Alopecia in which alopecia is caused by aggravation of atopic dermatitis is called atopic alopecia.
- atopic alopecia patients with filaggrin gene abnormality tend to have severe alopecia areata (Non-patent Document 7).
- lymphocytes infiltrate around the hair follicle, and eosinophils and mast cells also infiltrate.
- CD4 positive T lymphocytes account for 60 to 80%
- CD8 positive T lymphocytes account for 20 to 40%
- many HLA-DR positive cells and INF- ⁇ positive cells are found (Non-patent Document 8).
- Non-patent Document 9 there is also a report that the frequency of atopy and autoimmune disease in alopecia areata patients is not different from that of healthy individuals. Moreover, even though some relationship between alopecia areata and immune abnormality has been suggested, no specific causal relationship is known.
- Examples of drugs that can be used to treat alopecia areata include steroids such as diflorazone, betamethasone, dexamethasone, clobetasol, prednisolone, mometasone, methylprednisolone, deprodon, diflupredonate, fluocinonide, amsinonide, triamcinolone, difluprednate, hydrocortisone, Second-generation antihistamines such as azelastine, glycyrrhizin, methionine and glycine, glycyrrone (registered trademark), carpronium chloride, cephalanthin, minoxidil, cyclosporin A, katsushika kouryu oyster bath, half There are summer kobokuto, biotin, anthralin (disranol), tricyclic antidepressant and so on.
- steroids such as diflorazone, betamethasone, dexa
- alopecia areata
- local immunotherapy that modifies immunity by bringing the hair loss part into contact with a hair removal part by contacting a synthetic reagent called SADBE (squalic acid dibutyl ester) or DPCP (diphenylcyclopropenone), snowy carbonic acid or Cooling therapy with liquid nitrogen, linear polarized near-infrared radiation therapy (super riser therapy), PUVa therapy, a combination of psoralen and long-wave ultraviolet (UVA), stellate ganglion block, hypnosis, acupuncture Is done.
- SADBE synthetic reagent
- DPCP diphenylcyclopropenone
- UVA linear polarized near
- “Japanese Dermatological Association Alopecia Alopecia Clinical Practice Guidelines 2010 Edition” (Non-patent Document 10) has a recommendation level A (strongly recommended), recommendation level B (recommended to do), Evaluation is based on five levels: recommendation level C1 (you may consider doing it, but there is no sufficient basis), recommendation level C2 (not recommended because there is no basis), and recommendation level D (not recommended) ing.
- recommendation level A there is no treatment method of recommendation level A, and local steroid injection and local immunotherapy are listed as the treatment method of recommendation level B.
- the recommended degree of treatment is C1 for steroid pulse therapy by intravenous drip infusion for "adult patients with S2 or more that progress rapidly within 6 months after onset”, and for steroid pulse therapy for oral or internal steroid pulse therapy "S2 and higher adult cases” is recommended to use the second generation antihistamines as "one of the combination therapy for single and multiple cases with atopic predisposition", each with the recommended degree of C1.
- the guideline also states that cephalanthin, glycylone, topical steroids, topical carpronium chloride, topical minoxidil, cooling therapy, linearly polarized near-infrared radiation therapy, and PUVA therapy have not been fully demonstrated at this stage. However, it is classified into the recommendation degree C1 “considering medical treatment results”.
- Cyclosporin A and Keishika Karyukyo Oyakuto are classified into a recommendation degree C2 with a recommendation sentence “not recommended at present”. Furthermore, anthralin, tricyclic antidepressants, stellate ganglion block, and hypnosis are classified as recommendation level C2 with a recommendation of “do not use” or “do not do”. ing. Acupuncture is classified as a recommendation level D because it does not reach the level of medical evaluation.
- Non-patent Document 11 The prognosis of alopecia areata is low in the possibility of healing in cases where the baldness has a long duration or in cases where there is a history of atopic disease or autoimmune endocrine disease.
- Non-patent Document 12 According to reports from multiple institutions in Europe and the United States, 34 to 50% of all patients move to the all head type or the generalized type, and in that case, the recovery rate is very low, 10% or less (Non-patent Document 12 ). In adult cases with a hair loss area of less than 50%, 56% recovered, but with alopecia areata having a hair loss area of 50% or more, the recovery rate was only 3.7% (Non-patent Document 13).
- female pattern alopecia and its treatment method
- the growth period of hair is shortened and the rest period is prolonged due to the loss of hormone balance.
- the number of hairs coming out from one pore decreases, the hair itself becomes less than half that of a normal state, or the color of the hair becomes lighter.
- a state where the scalp from the gap hair around the crown portion becomes visible is observed as overall thinning pattern that is.
- Non-patent Document 25 states that the division of the division from the top of the head to the front of the head is considered to be important as an early symptom of female pattern baldness, based on the spread of branches of the Christmas tree. ing.
- Female pattern baldness is usually older than male pattern baldness and is often found in the 40s to 50s or after menopause. Since the administration of finasteride, which suppresses the activation of testosterone to dihydrotestosterone, was ineffective for menopausal women, the general idea that female thinning hair is not homogeneous with androgenetic alopecia. Thus, female pattern alopecia is diagnosed clearly from male pattern baldness based on gender, age, and diffuse alopecia.
- the cause of female pattern alopecia is caused by a decrease in estrogen due to menopause, as well as a decrease in female hormones due to rapid diet, stress, and withdrawal of oral contraceptives.
- Finasteride is virtually contraindicated in the treatment of female pattern alopecia because finasteride cannot be used for female pattern alopecia in women who are pregnant or breastfeeding. Minoxidil and cephalanthin are less effective against female pattern baldness. The effect of female pattern alopecia with female hormone replacement therapy is not known. Thus, there is no effective treatment method for female pattern alopecia.
- Seborrheic alopecia and method of treatment thereof In seborrheic alopecia, sebum is constantly secreted in large quantities from the pores, and the pores are blocked to the naked eye. Therefore, when the sebum is removed, the pores become red due to inflammation, and hair loss occurs due to this inflammation, so diagnosis is relatively easy.
- seborrheic alopecia The cause of seborrheic alopecia is thought to cause inflammation due to abnormal growth of resident bacteria of the scalp due to excessively secreted sebum, and by appropriately removing sebum from pores with a mild shampoo Although a certain therapeutic effect can be expected, it is difficult to maintain an appropriate sebum. In addition, it is said that the breeding of malassezia which is a kind of fungus is also contributed, and there may be a therapeutic effect by an antifungal agent for external use. Improvement is difficult and there is little cure for seborrheic alopecia.
- Alopecia areata is a disease in which dandruff becomes casabata-like, and a large amount of dandruff occurs abnormally enough to block pores and cause inflammation. Is relatively easy. The cause is said to be that abnormal bacteria on the scalp grow abnormally due to abnormal hormone balance, which leads to hair loss.
- steroid treatment is most effective among existing treatments, but this method takes time to complete, or treatment becomes difficult when symptoms become chronic It is not a recommended treatment because it is easy to fall into.
- Senile alopecia is alopecia in which hair loss and thinning occurs in the body hair of the whole body including the entire head with aging regardless of gender differences.
- the scalp is often dried and blood vessels can be seen through the skin.
- Treatment of senile alopecia is difficult because the body's ability to make new cells declines due to aging.
- the possibility of hair growth is improved by activating the hair papilla by massaging the scalp, etc., and there is no treatment method at all.
- Cancer chemotherapeutic alopecia is a cancer chemotherapeutic agent that selectively kills cancer cells that are actively dividing by cancer chemotherapeutic agents. Similarly, it is alopecia caused by damaging hair matrix cells in which cell division is active.
- Common names include, for example, cyclophosphamide, ifosfamide, doxorubicin, amrubicin, paclitaxel, docetaxel, irinotecan, epirubicin, etoposide, actinomycin D, bleomycin, vincristine, vinorelbine, carboplatin, methotrexate, cisplatin, melphalane, fluorouracil, fluorouracil, fluorouracil, It is known that alopecia is caused by chemotherapeutic agents such as capecitabine, tegafur, gimeracil, oteracil potassium, vinblastine, and ixaviberon.
- chemotherapeutic agents such as capecitabine, tegafur, gimeracil, oteracil potassium, vinblastine, and ixaviberon.
- cancer chemotherapeutic alopecia begins with the start of administration of a chemotherapeutic agent, and hair loss begins after 10 days, hair loss becomes conspicuous after 20 days, and all body hairs are lost after 30 to 60 days. .
- the recovery of body hair after the completion of cancer chemotherapy usually starts with 3-6 months after the end of administration of the chemotherapeutic agent, and the body hair almost recovers after about 8-12 months.
- cancer chemotherapeutic alopecia is caused by damage to hair matrix cells in the hair follicle by the cancer chemotherapeutic agent, so that the recovery of body hair after completion of cancer chemotherapy depends on the degree of damage of the hair matrix cells.
- the hair quality may drop, and the color of the hair and the thickness of the hair may change, and if it is severe, it may recover only to the way it grows.
- the body hair recovers, the state without body hair continues for a period of half a year to a year and a half, and during that period, the appearance changes drastically, coupled with anxiety about the cancer itself for the patient. It is a great pain.
- CTCAE Common Terminology Criteria for Adverse Events
- Cancer chemotherapeutic alopecia has no prevention or treatment. Therefore, until the cancer chemotherapeutic alopecia spontaneously recovers, there is only a coping method that makes the hair look natural by substituting the hair with a wig, writing eyebrows with eyebrows, and using eyelashes with eyelashes.
- alopecia areata, male pattern alopecia, female pattern alopecia, postpartum alopecia, seborrheic alopecia, critical alopecia, senile alopecia, cancer chemotherapeutic alopecia, respectively
- their treatment is also very limited.
- treatment with minoxidil or finasteride is recommended, but the effect is weak.
- natriuretic peptides As natriuretic peptides (NP; natriuretic peptide), three kinds of natriuretic peptide families are known. Specifically, atrial natriuretic peptide (ANP), B-type natriuretic peptide (BNP) B-type natriuretic peptide) and C-type natriuretic peptide (CNP), which are mainly known in the order of 28, 32 and 22 amino acids, respectively. .
- ANP atrial natriuretic peptide
- BNP B-type natriuretic peptide
- CNP C-type natriuretic peptide
- ANP and BNP ANP is synthesized primarily in the atria and BNP is synthesized primarily in the ventricle and is secreted from the heart to the whole body.
- ANP and BNP circulating in the blood are said to be almost 100% heart-derived. It has been reported that these ANP and BNP are deeply involved in pathological conditions such as hypertension, cardiac hypertrophy, heart failure, myocardial infarction, valvular disease, arrhythmia, and pulmonary hypertension.
- Human ANP is a peptide consisting of 28 amino acids that is produced and secreted by atrial cells. The 7th cysteine and the 23rd cysteine form a cyclic structure by disulfide bonds in the molecule. ANP exhibits diuretic action in the kidney and relaxes / expands vascular smooth muscle in blood vessels.
- human BNP is a peptide consisting of 32 amino acids produced and secreted by ventricular cells, and the 10th cysteine and the 26th cysteine form a cyclic structure by disulfide bonds in the molecule. BNP also has diuretic and vasodilatory effects.
- BNP is a peptide isolated and identified from pig brain in 1988 and is also called brain natriuretic peptide.
- Both ANP and BNP bind to the receptor NPR-A (also known as GC-A) having a guanylate cyclase domain, and promote the production of cGMP to express the above action.
- NPR-A also known as GC-A
- ANP promotes secretion in association with an increase in atrial fullness pressure in congestive heart failure or the like, and functions to reduce symptoms such as congestive heart failure by the above-described action.
- BNP also promotes secretion in the case of myocardial infarction, and functions to relieve various symptoms associated with myocardial infarction by the above-described action (Non-patent Document 14).
- the origin of BNP in the blood is mostly from the ventricle, but a part is also secreted from the atria.
- ANP hANP
- BNP congestive heart failure
- CNP Since CNP was first discovered in the brain, it was thought that it functions as a neuropeptide, but it was later revealed that it also exists in the periphery. In particular, in the vascular wall, smooth muscle cells have many CNP-specific receptors, and monocytes / macrophage cells and endothelial cells produce CNP. It is thought to be involved in the suppression of growth. From this, it is possible to prevent intravascular restenosis that occurs at a certain frequency and is clinically problematic after patients with ischemic heart disease undergo percutaneous coronary angioplasty (PTCA) by administration of CNP. The possibility of clinical application is currently being investigated.
- PTCA percutaneous coronary angioplasty
- CNP cardiac hypertrophy and fibrosis after myocardial infarction are markedly improved and cardiac function is improved.
- heart fibrosis causes diastolic dysfunction and arrhythmia
- CNP has a strong inhibitory effect on fibroblast proliferation, so research as a therapeutic agent for heart fibrosis has also been conducted.
- CNP is a hormone provided in the body, there is little concern about side effects, and it is expected to be applied as a clinical therapeutic agent for arteriosclerotic diseases and heart diseases.
- CNP-22 having 22 amino acids, CNP-53 having 53 amino acids with 31 amino acid residues added to the N-terminal thereof, and the like are known.
- Natriuretic peptide receptor NP receptors include NPR-A receptor having a guanylate cyclase domain (also known as GC-A), NPR-B receptor having a guanylate cyclase domain (also known as, GC-B), three types of receptors, NPR-C receptors that do not have a guanylate cyclase domain, are known, ANP is an NPR-A receptor and an NPR-C receptor, and BNP is an NPR- It is known that CNP can bind to the A and NPR-C receptors and the NPR-B and NPR-C receptors, respectively.
- NPR-A receptor activation of the NPR-A receptor results in vasodilatory action, diuretic action and cell growth inhibitory action.
- NPR-B receptors are abundant in vascular smooth muscle cells and are thought to bring about an inhibitory effect on the proliferation of vascular smooth muscle cells.
- the NPR-C receptor is also called a clearance receptor, and is thought to remove blood NP and regulate the concentration of tissue NP.
- natriuretic peptide has historically been first discovered as ANP as a peptide secreted by the atrium, and its vasodilatory action and diuretic action attracted attention. Later, BNP and CNP were found as peptides similar to ANP. From such historical background, attention has been focused on the relationship between the natriuretic peptide and immunity related to the cardiovascular system.
- Non-patent Document 15 CNP knockout mice show a dwarfism-like phenotype due to poor cartilage growth (Non-patent Document 15), and CNP can be expected to promote regeneration of articular cartilage. There is also interest in the relationship between and natriuretic peptides. However, this document does not describe the association between CNP and alopecia.
- ANP suppresses the secretion of macrophages by tumor necrosis factor ⁇ (TNF- ⁇ ) and interleukin 1 ⁇ (IL1 ⁇ ), which are inflammatory cytokines, suggesting a role in arthritis and sepsis (non-patent literature) 16).
- TNF- ⁇ tumor necrosis factor ⁇
- IL1 ⁇ interleukin 1 ⁇
- Non-patent Document 17 it has been reported that the BNP concentration in blood increases in parallel with rejection of heart transplantation, suggesting that it is involved in immune regulation in the cardiovascular system.
- this document does not describe the relationship between BNP and alopecia.
- Non-patent Document 18 Kuroski de Bold et al examined the immunoregulatory effect of natriuretic peptide, focusing on the increase in blood BNP concentration during rejection at heart transplantation. Both ANP and BNP suppress lymphocyte proliferation (Non-patent Document 18). However, this document does not describe the relationship between NP and alopecia.
- BNP is an inflammatory cytokine such as arachidonic acid, prostaglandin E2 (PGE2), leukotriene B4 ( LTB4) and interleukin 10 (IL10), which is an anti-inflammatory cytokine, both promote the release of macrophages, and thus have been reported to have some kind of inflammation-regulating action. It was not possible to conclude whether it worked or promoted (Non-patent Document 19). This document also does not describe the relationship between BNP and alopecia.
- PGE2 prostaglandin E2
- LTB4 leukotriene B4
- IL10 interleukin 10
- Non-patent Document 20 It has been reported that CNP is secreted from macrophages (Non-patent Document 20). In addition, Scotland et al reported that CNP suppressed platelet aggregation and leukocyte migration in the process of studying the role of CNP in myocardial injury after cardiac ischemia and reperfusion (Non-patent Document 21). . However, these documents do not describe the relationship between CNP and alopecia.
- CNP knockout mice exhibit a phenotype like dwarfism
- CNP is also of interest in relation to cartilage growth.
- Agoston et al has found that dexamethasone increases the expression of the CNP gene in primary cultured chondrocytes isolated from mouse fetal tibia (Non-patent Document 23).
- this document does not describe the relationship between CNP and alopecia.
- ANP ANP
- BNP CNP
- CNP CNP
- all of these documents include alopecia areata, androgenetic alopecia, sputum alopecia, postpartum alopecia, female pattern alopecia, seborrheic alopecia, alopecia, senile alopecia, etc.
- the association between a specific type of alopecia and natriuretic peptide is not described.
- none of these documents demonstrate that CNP or BNP is useful for the treatment of alopecia.
- CNP is used as a smooth muscle cell inhibitor, and does not suggest application of CNP or BNP to an alopecia treatment.
- Katsuhiko Nakata et al. Proposed an eye drop for promoting lacrimal secretion or treating keratoconjunctival disorders using natriuretic peptide as an active ingredient, and listed ANP, BNP and CNP as usable natriuretic peptides (Patent Document 2). .
- Kazukazu Nakao et al. Has proposed a composition for increasing height which is administered to an individual having no FGFR3 abnormality, comprising a guanylcyclase B (GC-B) activator such as CNP as an active ingredient (Patent Document 3). .
- GC-B guanylcyclase B
- CNP as a composition for increasing the height of CNP or BNP based on the finding that anal nasal length was greater than that of normal littermates in transgenic mice overexpressing CNP. It does not suggest the application to the therapeutic agent of alopecia.
- Kazukazu Nakao et al. Proposed a therapeutic or prophylactic agent for joint inflammation containing a guanyl cyclase B (GC-B) activator such as CNP as an active ingredient (Patent Document 4).
- GC-B guanyl cyclase B
- natriuretic peptide for the prevention of cirrhosis or liver cancer, and does not suggest the application of the natriuretic peptide to a therapeutic agent for alopecia.
- natriuretic peptide for the suppression of peritoneal fibrosis during peritoneal dialysis, and does not suggest the application of natriuretic peptide to a therapeutic agent for alopecia.
- Toshiyuki Hori et al. Have a GC-A receptor agonist as an active ingredient based on the fact that the proliferation of naive T cells induced by dendritic cells when LPS is added to the medium is suppressed by simultaneous addition of ANP.
- a prophylactic or therapeutic agent for Th1-type immune diseases has been proposed (Patent Document 10).
- tissue organ repair / regeneration preparation containing a composition that may contain a filler or an auxiliary agent has been proposed, and hair growth and hair growth is cited as an example of tissue organ repair / regeneration (Patent Document) 5).
- ANP was applied to the scalp of “54-year-old and 89-year-old men with thin hair” after shampooing twice a day.
- Patent Document 5 describes only hair growth by ANP, and does not demonstrate any hair growth and hair growth by CNP and BNP.
- alopecia based on various causes of alopecia, and even though treatment methods are completely different from each other, what type of alopecia is merely described as “54-year-old and 89-year-old male with thin hair” It is unclear whether the effect was seen in alopecia, and the feature that “the front row of the head hair that was receding moves forward” is a feature that is seen in various alopecias, so what only with these descriptions is It is impossible to know if the hair is thin due to the cause or disease.
- this document only contemplates a “hair growth and hair growth preparation” as a very broad concept, and it is also unclear whether it is a therapeutic agent or a preventive agent, and a specific therapeutic agent or preventive agent for alopecia It is not pronounced, nor is it a therapeutic or prophylactic agent for dandruff, gray hair and seborrheic scalp.
- the literature includes alopecia areata, male pattern alopecia, postpartum alopecia, female pattern alopecia, seborrheic alopecia, critical alopecia, senile alopecia, cancer chemotherapeutic alopecia, It is clear that it does not evoke a therapeutic or prophylactic agent for alopecia, dandruff, gray hair, and seborrheic scalp due to radiation exposure.
- ANP and BNP both act as hormones secreted from the heart into the blood and act as neurotransmitters and are thought to play an important role in maintaining body fluid volume and blood pressure homeostasis (Omitted)
- CNP has a similar primary amino acid sequence to ANP and BNP, and natriuretic action and blood pressure lowering when administered in vivo.
- CNP is an NP family It occupies a specific position, and its physiological role is more than maintaining fluid volume and blood pressure homeostasis. (Omitted) Comparing the structure of CNP with those of ANP and BNP reveals that CNP differs from ANP or BNP in the following points ( That is, the primary amino acid sequence of CNP is completely different from ANP or BNP in the exocyclic N-terminal domain, and in the endocyclic domain, 5 residues are ANP and 4 residues are BNP out of 17 amino acid residues.
- the structure of the exocyclic C-terminal domain of CNP is very different from that of ANP or BNP, and CNP does not have the tail structure that exists in ANP or BNP (in the case of ANP / BNP, it is cyclic) (5 ANP and 6 BNP amino acid residues are added to the C-terminal side of the structure, and this structure is called tail structure for convenience) It is clear that the structural differences between CNP and ANP or BNP described above are involved in the above-described expression of the characteristic pharmacological action of CNP. "
- Betz RC Loss-of-function mutations in the filaggrin gene and alopecia areata: strong risk factor for a severe course of disease in patients comorbid for atopic disease .J543Invest Dermatol.-2 Norio Katsuoka: Atopic disease and alopecia areata-Atopic alopecia--Derma 23, 9-12, 1999 Serarslan G, et al., Is atopy and autoimmunity more prevalent in patients with alopecia areata? A comparative study. J Eur Acad Dermatol Venereol. Doi: 10.1111 / j.1468-3083.2011. Japanese Dermatological Association Alopecia Alopecia Practice Guidelines 2010 (Journal of Japanese Dermatological Association: 120 (9), 1841-1859, 2010)
- Kiemer A.K. Vollmar A.M., Annals of the Rheumatic Disease, The atrial natriuretic peptide regulates the production of inflammatory mediators in macrophages. 60: iii68-iii70.2001 Meirovich Y.F ,, et al., Relationship between natriuretic peptides and inflammation: proteomic evidence obtained during acute cellular cardiac allograft rejection in humans. TheourJournal of Heart and Lung Transplantation.
- C-type natriuretictripeptide is synthesized and secreted from leukemia cell lines, peripheral blood cells, and peritoneal macrophages.
- Alopecia causes serious mental distress due to appearance problems, but no conclusive treatment has been found.
- minoxidil or finasteride does not provide a sufficient therapeutic effect, and for alopecia areata there is no effective treatment method.
- Alopecia areata is a flammable disease as well as an intractable disease, and its appearance is remarkably impaired and can cause depression, so it needs to be treated.
- Postpartum alopecia in combination with postpartum depression, because of the loss of a large amount of body hair within a short period of time after parturition, there is no treatment even though the patient's mental burden is great.
- Female pattern alopecia, seborrheic alopecia, critical alopecia and senile alopecia are poorly recognized and still have no treatment.
- Cancer chemotherapeutic alopecia is a sudden loss of whole body hair, and the condition persists for a long period of time, so even though the patient's upset is great, the treatment is equally good, and the treatment of cancer Therefore, development of treatment methods is strongly desired.
- Alopecia due to radiation exposure is the same as cancer chemotherapy-induced alopecia.
- the object of the present invention is to provide alopecia patients, in particular alopecia areata, androgenetic alopecia, postpartum alopecia, female pattern alopecia, seborrheic alopecia, critical alopecia, senile alopecia, Not only is it effective and safe against cancer chemotherapeutic alopecia and alopecia due to radiation exposure, it also has no side effects such as pruritus, irritation and feminization, no contraindications, and relapses even after discontinuation of use. It is to provide a new therapeutic agent for alopecia.
- the purpose of the present invention is, regardless of whether the cause of these alopecias, ie, male hormones, female hormones, their balance, any immune abnormality, inflammation, aging, cancer chemotherapeutic agents, New therapeutic agent and / or preventive agent for alopecia having hair growth / hair growth / hair increase effect, white hair treatment effect and hair thickening effect, and treatment agent and / or preventive agent for dandruff, white hair and seborrheic scalp Is an offer.
- alopecias ie, male hormones, female hormones, their balance, any immune abnormality, inflammation, aging, cancer chemotherapeutic agents, New therapeutic agent and / or preventive agent for alopecia having hair growth / hair growth / hair increase effect, white hair treatment effect and hair thickening effect, and treatment agent and / or preventive agent for dandruff, white hair and seborrheic scalp Is an offer.
- type A natriuretic peptide which is known as a therapeutic agent for acute heart failure
- type B natriuretic which is known as a therapeutic agent for congestive heart failure
- Peptide (BNP) and C-type natriuretic peptide (CNP) which has been conventionally known as a vascular smooth muscle growth inhibitor, is excellent as a therapeutic and / or preventive agent for alopecia, dandruff, gray hair and seborrheic scalp It has been found to have effectiveness and safety.
- the therapeutic agent for alopecia of the present invention is, in particular, alopecia areata, male pattern alopecia, postpartum alopecia, female pattern alopecia, seborrheic alopecia, critical alopecia, senile alopecia, cancer chemotherapy Excellent efficacy and safety against alopecia areata and alopecia due to radiation exposure.
- the therapeutic agent for alopecia of the present invention is a conventional treatment method, which is a steroid agent, an antihistamine agent, glycyrone (registered trademark), carpronium chloride, cephalanthin, minoxidil, finasteride, cyclosporin A, Keishika Karyukyou oyster, half It has a clear therapeutic effect on alopecia that is resistant to treatment with Natsukobokuto, biotin, anthralin, local immunotherapy, cooling therapy, linear polarized near-infrared irradiation therapy, and PUVA therapy, The present invention was completed by confirming that there was no side effect such as irritation and feminization, and that there was no immediate relapse after discontinuation of use.
- a combination of CNP or BNP with betamethasone valerate and gentamicin sulfate, a combination of CNP or BNP with clobetasol propionate, a combination of CNP with carpronium chloride, and CNP or BNP with minoxidil Combined multi-layer application, male pattern alopecia other than alopecia areata, postpartum alopecia, female pattern alopecia, seborrheic alopecia, critical alopecia, senile alopecia, cancer chemotherapeutic alopecia
- the present invention was completed by confirming that black bristles grew against alopecia due to radiation exposure.
- the present invention is specifically as follows. [1] Treatment or prevention agent for alopecia, dandruff, pruritus, gray hair and seborrheic scalp containing natriuretic peptide (NP) as an active ingredient, hair growth agent, hair restorer, hair loss progression preventive agent, hair loss progression preventive agent Agents, hair growth promoters, hair growth promoters, hair nourishing agents, post-birth or post-hair loss treatment or prevention agents.
- NP natriuretic peptide
- Alopecia is alopecia areata, male pattern alopecia, postpartum alopecia, female pattern alopecia, seborrheic alopecia, critical alopecia, alopecia, cancer chemotherapeutic alopecia, elderly
- the therapeutic or prophylactic agent according to [1], which is alopecia areata or alopecia caused by a drug.
- natriuretic peptide is any of a CNP derivative, a BNP derivative, or an ANP derivative.
- NP is any of C-type natriuretic peptide (CNP), B-type natriuretic peptide (BNP), or A-type natriuretic peptide (ANP) or Preventive agent.
- a natriuretic peptide (NP) is a CNP derivative, CNP-22, or CNP-, in which any amino acid is deleted, substituted or added in the amino acid sequence of CNP-22 or CNP-53 and has CNP activity 53.
- NP natriuretic peptide
- ANP28 A-type natriuretic peptide
- BNP derivative BNP derivative in which any amino acid is deleted, substituted or added in the amino acid sequence of ANP28 and has BNP activity
- ANP28 A-type natriuretic peptide
- BNP derivative BNP derivative in which any amino acid is deleted, substituted or added in the amino acid sequence of ANP28 and has BNP activity
- the natriuretic peptide is a chimeric peptide of two or more natriuretic peptides (NP) selected from ANP, BNP or CNP, wherein a cyclic structure is formed by an intramolecular disulfide bond,
- the BNP is BNP-26, BNP-32, BNP-45, or any arbitrary sequence of 5 amino acids or more in the amino acid sequence of BNP-26 from which any one to 5 amino acids have been deleted, substituted or added.
- the ANP is a peptide comprising ANP or an arbitrary amino acid sequence of 5 or more amino acids in the amino acid sequence of ANP in which 1 to 5 arbitrary amino acids are deleted, substituted or added;
- the therapeutic or prophylactic agent according to [1] which is a chimeric peptide having CNP activity, BNP activity or ANP activity, or a derivative of the above-mentioned NP chimeric peptide.
- [12] Further comprising at least one steroid selected from the group consisting of diflorazone, betamethasone, dexamethasone, clobetasol, prednisolone, mometasone, methylprednisolone, deprodon, diflupredonate, fluocinonide, amsinonide, triamcinolone, difluprednate, hydrocortisone.
- steroid selected from the group consisting of diflorazone, betamethasone, dexamethasone, clobetasol, prednisolone, mometasone, methylprednisolone, deprodon, diflupredonate, fluocinonide, amsinonide, triamcinolone, difluprednate, hydrocortisone.
- at least one antihistamine selected from the group consisting of azelastine, oxatomide, fexofenadine, emedastine, ebastine, cetirizine, bepotastine, olopatadine, and loratadine.
- the therapeutic or prophylactic agent according to [2], wherein the male pattern baldness is Hamilton-Norwood type Va, VI or VII.
- the therapeutic or prophylactic agent according to [1], wherein the alopecia areata is normal alopecia, total alopecia, generalized alopecia or serpentine alopecia.
- alopecia is alopecia in a subject having a history or a combination of allergic diseases or autoimmune diseases.
- Autoimmune diseases are chronic discoid lupus erythematosus, localized scleroderma, pemphigus, pemphigoid, gestational herpes zoster, linear IgA bullous dermatosis, acquired epidermolysis bullosa, vulgaris vulgaris, Sutton
- the therapeutic agent or prophylactic agent according to [29] which is any of acquired centrifugal vitiligo.
- the alopecia is alopecia in a subject having a history or complication of autoimmune thyroid disease, common vitiligo, systemic lupus erythematosus, rheumatoid arthritis, or myasthenia gravis A therapeutic or prophylactic agent.
- alopecia is alopecia in a subject having a history or complication of atopic dermatitis or allergic rhinitis.
- alopecia is alopecia in a subject having a filaggrin gene abnormality and having a history or a combination of atopic dermatitis.
- the alopecia is alopecia in a subject exhibiting an allergic reaction to at least one allergen selected from the group consisting of house dust, mites, cedar, camogaya, ragweed, and cat hair. A therapeutic or prophylactic agent.
- Alopecia is a group consisting of house dust, ticks, cedar, camouflage, ragweed, and cat hair in any allergen test of scratch test, intradermal test, patch test, specific IgE antibody in vitro measurement method
- the therapeutic or prophylactic agent according to [1] which is alopecia in a subject exhibiting an allergic reaction to at least one allergen selected from *
- Alopecia is a steroid, antihistamine, Glycylon (registered trademark), carpronium chloride, cephalanthin, minoxidil, finasteride, cyclosporin A, Keishige Karyu bone oyster bath, Hanka Kobokuto, biotin, anthralin, local immunotherapy, cooling
- alopecia alopecia showing a treatment-resistant to steroid treatment agent, a therapeutic agent or prophylactic agent according to [1].
- alopecia alopecia showing a treatment-resistant to steroid treatment agent, a therapeutic agent or prophylactic agent according to [1].
- the therapeutic or prophylactic agent according to [1] wherein the alopecia is alopecia in a subject who has reached a difficult steroid withdrawal state.
- alopecia is alopecia exhibiting treatment resistance to stimulation therapy with liquid nitrogen.
- the therapeutic or prophylactic agent according to [2], wherein the alopecia areata is S1 or B0 or more alopecia.
- the therapeutic or preventive agent according to [2], wherein the alopecia areata is S2 or more alopecia.
- the therapeutic or prophylactic agent according to [2], wherein the alopecia areata is S3 alopecia or more.
- the therapeutic or prophylactic agent according to [2], wherein the alopecia areata is S4 or more alopecia.
- the therapeutic or prophylactic agent according to [2], wherein the alopecia areata is S5 or more alopecia.
- the therapeutic or prophylactic agent according to [2], wherein the alopecia areata is B0 alopecia.
- the dosage form is an ointment, gel, cream, lotion, liquid, wax, powder or spray, gel spray, foam, shampoo, treatment, scalp treatment, or tonic
- the therapeutic or prophylactic agent according to [1] which is an agent.
- NP natriuretic peptide
- NP natriuretic peptide
- the therapeutic agent or prophylactic agent according to [1] the therapeutic agent or prophylactic agent according to [1].
- the therapeutic or prophylactic agent according to [1], wherein the content of natriuretic peptide (NP) is 20 to 300 ⁇ g / g.
- Alopecia is a decrease in pituitary function, endocrine abnormalities such as hypothyroidism or enhancement, nutritional disorders, hypoalbuminemia, cachexia, iron deficiency anemia, zinc deficiency, homocystinuria, cirrhosis, etc.
- the therapeutic agent or prophylactic agent as described in.
- the therapeutic agent of the present invention containing natriuretic peptide (NP) as an active ingredient is alopecia areata, male pattern alopecia, female pattern alopecia, seborrheic alopecia, acupuncture Alopecia, postpartum alopecia, senile alopecia and cancer chemotherapeutic alopecia can be markedly improved.
- the therapeutic agent of the present invention can restore gray hair to black hair or the original color. Furthermore, if the therapeutic agent of the present invention is used, dandruff is reduced.
- the therapeutic agent of the present invention has no side effects such as pruritus, irritation and feminization, and does not relapse for alopecia areata and cancer chemotherapeutic alopecia for at least half a year even if it is stopped. .
- the therapeutic agent of the present invention is useful as a very effective therapeutic agent for male pattern alopecia in which sufficient treatment effect cannot be obtained by conventional minoxidil or finasteride, and alopecia areata having no effective treatment method. Sex can be expected.
- the therapeutic agent of the present invention is equivalent to no treatment, female pattern alopecia, seborrheic alopecia, erosion alopecia, postpartum alopecia, senile alopecia, cancer chemotherapeutic alopecia In addition to alopecia due to radiation exposure, it has a remarkable hair growth / hair growth / hair increase effect and can dramatically reduce the amount of hair loss and prevent the progress of hair loss.
- the therapeutic agent of the present invention can convert a miniature hair root into a hair root that grows large, hardened hair, and can make the hair quality harder and thicker.
- the therapeutic agent of the present invention also promotes hair growth, prolongs the growth period, and increases long hair.
- the therapeutic agent of the present invention promotes hair growth and hair elongation, and increases the hair elongation rate.
- the therapeutic agent of the present invention can increase the number of hairs per hair follicle.
- the therapeutic agent of the present invention promotes hair growth and hair growth in the refractory frontal region or M-type region, and is classified into Va, VI, and VII according to the Hamilto-Norwood classification, which is a wide range of severe androgenetic alopecia Alopecia also has a hair growth effect, a hair growth effect, and a hair growth effect.
- the therapeutic agent of the present invention regenerates the hair, and the newly born hair does not fall off even after the application is stopped, and has the effect of preventing the fallen hair.
- the therapeutic agent of the present invention can dramatically improve severe alopecia of the adult head, which is particularly difficult to treat and interferes with social life, without any side effects.
- the therapeutic agent of the present invention is not only effective for refractory alopecia but also exhibits the same effect regardless of gender, adults and minors.
- the treatment plan by Western specialists with minoxidil and finasteride is only for types II to V of the Hamilton-Norwood classification (Non-patent Document 24), and hair is considered to be ineffective for the types Va, VI and VII of the Hamilton-Norwood classification.
- the hair loss is dramatically reduced in the Hamilton-Norwood types Va, VI, and VII types, the growth period is prolonged, the long hair is increased, the hair is raised, the hair is thick and dark, and the hair is raised.
- the effect of improving hair growth is accelerated, the stretching speed is increased, black hair is increased, hair growth is improved, and white hair is improved within 1 to 3 weeks after application.
- conventional steroid local injection used for alopecia areata has the disadvantage that skin atrophy occurs at the site of local injection, requiring a large number of local injections and the total amount of injection when hair loss is extensive.
- the local immunotherapy for alopecia areata has the problem that adverse events such as systemic contact alopecia, local lymphadenopathy, and mechanical urticaria can occur.
- the present invention not only this defect is not seen at all, excellent effect that hair loss is renewed, the effect of treating alopecia is not lost for a long time after use is stopped, and the loss of regenerated hair is prevented. Was confirmed.
- good skin condition persisted for more than half a year even after discontinuation of application for alopecia areata and cancer chemotherapeutic alopecia.
- the therapeutic agent of the present invention comprising ANP, BNP, CNP, derivatives of these NPs, two or more NP chimeric peptides selected from these NPs, or derivatives of these NP chimeric peptides as active ingredients It also showed therapeutic effects on alopecia areata, which was resistant to steroids, cooling therapy, antiallergic agents, carpronium chloride, and cephalanthin.
- the therapeutic agent of the present invention comprising BNP, CNP, derivatives of these NPs, chimeric peptides of these NPs, or derivatives of these NP chimeric peptides as active ingredients is intractable circular hair loss having a large hair loss area.
- the therapeutic agent of the present invention contains CNP or BNP as an active ingredient
- the amount of hair loss dramatically decreases from about 3 days after application, and once or twice a day for 1 to 2 weeks.
- the hair grows by application, and in many cases, the background becomes difficult to see after 4 weeks of application. After that, even if it does not continue to be applied, the hair continues to grow and becomes hard hair and heals.
- the effect of the therapeutic agent of the present invention containing CNP or BNP as an active ingredient is strong, and hair growth is remarkably recovered even in the case of alopecia areata-type alopecia areata which is extremely refractory.
- the therapeutic agent of the present invention containing CNP as an active ingredient can more reliably suppress inflammation at the hair loss site than when BNP is used as an active ingredient, and symptoms such as erythema, scales, and crusts are short-term. Will be improved.
- the therapeutic agent of the present invention containing CNP as an active ingredient has a stronger effect of reducing the amount of hair loss than when BNP is used as an active ingredient, suppresses pruritus, and causes hair growth earlier.
- the hair growth effect continues for a longer period of time after the application is stopped and continues to increase. Therefore, CNP is most recommended when there are inflammatory symptoms such as erythema and scale on the scalp at the hair loss site.
- the therapeutic agent of the present invention can cause hair growth while suppressing inflammation of seborrheic alopecia and erosion alopecia.
- the therapeutic agent of the present invention promotes hair regeneration and dramatically reduces hair loss even in female pattern alopecia, postpartum alopecia, senile alopecia, cancer chemotherapeutic alopecia and alopecia due to radiation exposure. Hair can be raised, hair thickened, thickened, hair grown, hair stretch promoted, stretch speed increased, and long hair increased.
- the therapeutic agent of the present invention suppresses skin inflammation, chronic discoid lupus erythematosus, localized scleroderma, pemphigus, pemphigoid, gestational herpes zoster, linear IgA bullous dermatosis, acquired epidermolysis bullosa
- hair can be produced at a hair loss site of a subject having a history or complication of an autoimmune disease associated with skin symptoms such as vitiligo vulgaris or Sutton acquired efferent vitiligo.
- alopecia areata may be associated with autoimmune diseases, but the therapeutic agent of the present invention is used for autoimmune thyroid disease, vitiligo vulgaris, systemic lupus erythematosus, indirect rheumatism, myasthenia gravis. Hair growth can be caused at a hair loss site of a subject with a history or complication of an autoimmune disease such as symptom.
- the therapeutic agent of the present invention suppresses inflammation and improves the skin condition of the scalp, so that endocrine abnormalities such as hypopituitarism, hypothyroidism or enhancement, nutritional disorders, hypoalbuminemia, cachexia Quality, iron deficiency anemia, zinc deficiency, homocystinuria, alopecia due to metabolic disorders such as cirrhosis, resting alopecia due to high fever, labor, major surgery, antithyroid, anticoagulant, antitumor agent, thallium, It is also effective for drug-induced alopecia with psychotropic drugs and ⁇ -blockers.
- endocrine abnormalities such as hypopituitarism, hypothyroidism or enhancement, nutritional disorders, hypoalbuminemia, cachexia Quality, iron deficiency anemia, zinc deficiency, homocystinuria
- alopecia due to metabolic disorders such as cirrhosis, resting alopecia due to high fever, labor, major surgery, antithyroid, anticoagul
- NPR-C receptor common to NP is considered to be a clearance receptor that does not mediate pharmacological action.
- ANP and BNP are said to bring about vasodilatory, diuretic and cell growth-inhibiting effects by activating NPR-A receptor, and CNP inhibits vascular smooth muscle cell proliferation by activating NPR-B receptor.
- the action of CNP is expected to be different from that of BNP and ANP because it is believed to produce an action.
- the therapeutic agent of the present invention containing CNP or BNP as an active ingredient is clearly In particular, the therapeutic effect is higher than when ANP is used as the active ingredient, and in particular, the therapeutic effect is higher when CNP is used as the active ingredient.
- the therapeutic agent of the present invention containing BNP as an active ingredient is characterized in that black hard hair often grows.
- Natriuretic peptide (NP) which is an active ingredient of the present invention, is a hormone originally provided in the body, has little side effects even when applied to the skin, and is considered to have a minor effect on hemodynamics as long as it is used appropriately. In addition, since it can be used with peace of mind even for patients with low or unstable blood pressure, long-term administration is possible even for patients with chronic alopecia.
- alopecia areata and cancer chemotherapeutic alopecia
- alopecia does not recur at the site of application even after discontinuation of administration.
- the therapeutic agent of the present invention has an advantage that it can be used for children and women, and it is an extremely superior therapeutic agent that has never been used before.
- the amino acid sequence of human CNP peptide and the amino acid sequence of human BNP peptide and human ANP peptide include an amino acid sequence represented by “CFG”, an amino acid sequence represented by “DRI”, an amino acid sequence represented by “SGLGC”, These three common regions have four different sequences separated by these three common sequences.
- ANP gel agent The severity of alopecia areata was evaluated by the ratio of the bald area to the entire head based on the guidelines for evaluation of alopecia areata in the United States, and was compared for each case before and after application of the ANP gel. Each point on the left indicates the severity before application, and each point on the right indicates the severity after application. Each point indicating the severity of the same subject before application and the severity after application is connected by a straight line.
- ANP gel only in cases where no irritation symptoms occur, there are rare cases where a certain effect has been shown in the treatment of alopecia areata. Then itchy.
- ANP gel erythema, scales, itchiness, dandruff became severe and hair loss increased, and in most cases, the use was stopped. This tendency was particularly noticeable in male pattern baldness. It was.
- T2 is the same site after the 100 ⁇ g / g CNP ointment was applied twice a day for 2 weeks and the next day 100 ⁇ g / g ANP gel was applied twice a day for 5 weeks. Show. Stronger hair growth was observed before application and in FIG. 8 compared with T1.
- T2 is the bald patch of the same site after applying 100 ⁇ g / g BNP gel twice a day for 23 days
- T3 is 5 months after application of 100 ⁇ g / g BNP gel was stopped in 24 days
- Each subsequent bald patch of the same site is shown. Hair growth was observed such that the location of the bald patch was almost unknown, and hair growth continued even after application was stopped.
- FIG. 1 It is a drawing substitute photograph which shows the therapeutic effect at the time of apply
- the subject is facing downward in the photo.
- P is the bald patch before application
- T1 is the bald patch of the same site after applying 100 ⁇ g / g BNP gel twice a day for 2 weeks
- T2 is 100 ⁇ g / g BNP gel per day 2
- T3 indicates the bald patch of the same site after 3 weeks of application
- T3 indicates the bald patch of the same site after 3 weeks after application of 100 ⁇ g / g BNP gel was stopped. Remarkable hair growth and thickening were observed.
- T2 was obtained by applying 50 ⁇ g / g BNP ointment twice a day for 2 weeks, and then applying 30 ⁇ g / g BNP ointment twice a day for 1 week, and then adding 50 ⁇ g / g BNP.
- the bald patch of the same site after applying the ointment twice a day for 2 weeks is shown respectively.
- T1 in FIG. 15-1 further remarkable hair growth and thickening were observed.
- T3 is a bald patch of the same site after 100 ⁇ g / g CNP ointment was applied twice a day for 1 week, and from the next day 100 ⁇ g / g CNP gel was applied twice a day for 3 weeks Are shown respectively. Clear hair growth and expansion of the hair growth range were observed.
- P is the bald patch before application
- T1 is the bald patch of the same site after applying 50 ⁇ g / g BNP gel twice a day for 3 days
- T2 is the 50 ⁇ g / g BNP gel once a day
- the bald patch of the same site after application for 21 days is shown respectively. Clear hair growth and hair growth was observed.
- the scalp of the scalp within the frame surrounded by the dotted line is visible, and only a very thin white hair such as vellus hair grows, whereas in T, the hair loss in the frame surrounded by the dotted line. Black hair is dense on the scalp.
- FIG. 1 It is a drawing substitute photograph which shows the therapeutic effect at the time of apply
- the subject is facing downward in the photo.
- P represents a thin hair site before application
- T represents a hair loss site of the same site after 50 ⁇ g / g BNP gel was applied twice a day for 2 weeks.
- the hair growth at the hair loss site is sparse and the hair is thin, whereas in T, the hair growth is dense and the hair is thick and firm.
- attention is paid to the background of the M-shaped part it can be seen that hair growth is dense.
- the hair at the hair loss site in the frame surrounded by the dotted circle is sparse, whereas in T1, the hair with a sense of volume is dense in the center of the frame surrounded by the dotted circle, and T2 Then, the hair grows dense so that the so-called M-type hair loss site disappears.
- T2 the so-called O-shaped hair loss site in the center of the frame surrounded by a dotted circle is conspicuous, so that the top of the head, which is the remaining hair loss site, can be seen well. Because it was taken from the camera angle.
- the subject is facing downward in the photo.
- P represents the hair loss site before application
- T represents the same site after 50 ⁇ g / g BNP gel was applied twice a day for 1 week.
- the P photograph shows a sparse scalp, whereas the T photograph shows hair growth on the scalp.
- FIG. 1 It is a drawing substitute photograph which shows the therapeutic effect at the time of apply
- the subject is facing downward in the photo.
- P is the thin hair portion before application
- T1 is the thin hair portion after 100 ⁇ g / g ANP gel was applied twice a day for 3 weeks
- T2 is 50 ⁇ g from the day after the application of the ANP gel was completed for 1 week.
- coating a CNP gel of / g twice a day for 4 weeks is shown, respectively. After applying the CNP gel, apparent hair thickening was seen in the frontal region, and hair loss disappeared.
- FIG. 1 It is a drawing substitute photograph which shows the therapeutic effect at the time of apply
- the subject is facing downward in the photo.
- P represents a hair loss site before application
- T represents the same site after a CNP gel with a concentration of 50 ⁇ g / g was applied twice a day for 6 weeks from the front to the top of the head.
- the number of hairs increased at the hair removal site to which the CNP gel was applied, and considerable hair growth was observed. The hair became thicker and hair elongation was confirmed.
- a photo which substitutes for a drawing, showing the therapeutic effect when a 50 ⁇ g / g CNP: 600 ⁇ g / ml betamethasone: 500 ⁇ g / ml gentamicin combination is applied to a circular hair loss spot on the left temporal region of a case of cancer chemotherapeutic alopecia C35 It is.
- the subject is facing the left of the photo.
- P represents the hair loss site before application
- T represents the same site after 50 ⁇ g / g CNP: 600 ⁇ g / ml betamethasone: 500 ⁇ g / ml gentamicin combination was applied twice a day for 3 weeks. Remarkable hair growth was confirmed in the bald area to which the CNP gel was applied.
- the present invention relates to alopecia areata, male pattern alopecia, seborrheic alopecia, critical alopecia, female pattern alopecia, postpartum alopecia, senile alopecia, cancer chemotherapeutic alopecia and radiation exposure
- NP natriuretic peptide
- alopecia areata refers to alopecia that is generally clinically diagnosed as alopecia areata, and is not particularly limited.
- a subject with a history or complication of an immune disease, or an immune disease This refers to alopecia that suddenly develops in subjects with a genetic background.
- Alopecia areata as used herein includes, but is not limited to, alopecia that is typically clinically diagnosed as alopecia areata. In subjects with immune system overreactivity or abnormalities, an excess of immune system Includes all alopecias for which the cause other than having a response or immune abnormality is unknown.
- Alopecia generally diagnosed clinically as alopecia areata is a case where a bald area with a sharp outline from a coin-sized circle appears suddenly without subjective symptoms or prodromal symptoms and does not heal spontaneously. It is alopecia that expands its scope and becomes intractable.
- Alopecia, which is generally clinically diagnosed as alopecia areata shows cut hairs, eyelashes (spots in hair follicles) and easily removed hairs inside and outside the lesion during the active period.
- the decisive factor in the diagnosis is that the form resembles the shape of an exclamation mark.
- immune diseases refer to diseases caused by excessive reactions of the immune system or immunity abnormalities, including allergic diseases and autoimmune diseases.
- Immune system overreaction or immune abnormality refers to an excessive or abnormal immune response that causes the subject's own normal cells to be impaired, and specifically includes allergic and autoimmune diseases .
- An immune system overreaction or immune abnormality can be recognized as a history or complication of an immune disease.
- a subject having an immune system overreaction or an immune abnormality is synonymous with alopecia having a history or complication of an immune disease.
- a subject having a genetic background of an immune disease refers to a subject having a genetically linked family member who has an excessive immune system reaction or immune abnormality.
- Alopecia areata is known to occur at a high frequency when a family member with genetic illness has an immune disease, and the cause is unknown in subjects with a genetic background of immune disease Alopecia can be regarded as alopecia areata.
- At least the blood-connected parents, blood-connected brothers, blood-connected grandparents, blood-connected children or blood-connected grandchildren have allergic or autoimmune diseases.
- a person who has a history or a merger is determined to be a subject having a genetic background of immune disease.
- a subject with a genetic background of alopecia areata. Judge that there is.
- allergic diseases include atopic disease, hay fever, food allergy, latex allergy, metal allergy, sick house syndrome, allergic granulomatous vasculitis, food-dependent exercise-induced anaphylaxis, and celiac disease.
- atopic diseases include bronchial asthma, atopic dermatitis, allergic rhinitis, and atopic alopecia.
- Atopic alopecia refers to a condition in which alopecia is caused by aggravation of atopic dermatitis.
- a subject having an atopic predisposition means at least one of a person or a blood connected parent, a blood connected brother, a blood connected grandparent, a blood connected child or a blood connected grandchild.
- allergens that cause allergic reactions include house dust, ticks, cedar, camouflage, ragweed, and cat hair.
- cedar, camouflage, and ragweed here mean the cedar pollen, the camphor pollen, and the ragweed pollen, respectively.
- Autoimmune diseases include Hashimoto's disease, Graves' disease, autoimmune thyroid diseases such as primary hypothyroidism, vitiligo vulgaris, systemic lupus erythematosus, rheumatoid arthritis, myasthenia gravis, chronic discoid lupus erythematosus, limited Scleroderma, pemphigus, pemphigoid, gestational herpes zoster, linear IgA bullous dermatosis, acquired epidermolysis bullosa, Sutton acquired efferent vitiligo, Guillain-Barre syndrome, chronic atrophic gastritis, autoimmunity Hepatitis, primary biliary cirrhosis, primary sclerosing cholangitis, autoimmune pancreatitis, aortitis syndrome, Goodpasture syndrome, rapidly progressive glomerulonephritis, megaloblastic anemia, autoimmune hemolytic anemia, self Immun
- autoimmune diseases include chronic discoid lupus erythematosus, localized scleroderma, pemphigus, pemphigoid, gestational herpes zoster, linear IgA bullous dermatosis, acquired epidermolysis bullosa, vulgaris vulgaris And Sutton acquired efferent vitiligo. Autoimmune diseases that show skin symptoms are likely to be associated with alopecia.
- autoimmune diseases include those that are likely to be associated with alopecia areata.
- autoimmune diseases that are particularly likely to be associated with alopecia areata include autoimmune thyroid disease, vitiligo vulgaris, systemic lupus erythematosus, indirect rheumatism, and myasthenia gravis (Non-patent Document 8).
- male pattern alopecia refers to a symptom in which the hair on the frontal region and / or the top of the head gradually becomes soft and thins over several years in an adult male or female.
- male pattern baldness as described in the “Male Pattern Alopecia Practice Guidelines 2010 Edition” (Non-Patent Document 2), a relatively wide range of the top of the head can be used even for women. It develops as a pattern of thinning hair.
- Androgenetic alopecia occurs in subjects with a genetic background of androgenetic alopecia because hair papillae cells in the frontal or parietal scalp respond to 5 ⁇ dihydrotestosterone and miniaturize the hair follicles. If the frontal and / or parietal hair gradually softens and thins over several years, it is male pattern baldness.
- Having a genetic background of androgenetic alopecia means having a genetic background in which androgen acts on androgen-sensitive hair follicles, and specifically, the scalp on the frontal or parietal region.
- there is a related male who is in a grandparent, a blood-connected child, or a blood-connected grandchild who has a hair in the frontal or parietal region after 20 years old and the scalp is visible.
- critical alopecia means critical alopecia in the normal medical sense, and alopecia caused by dandruff closing pores and causing inflammation is included in critical alopecia. It is.
- female pattern alopecia means female pattern alopecia in the usual medical sense, and alopecia caused by a decrease in the amount of the female hormone estrogen relative to the amount of androgens in the bloodstream, Included in female pattern alopecia.
- postpartum alopecia means postpartum alopecia in the usual medical sense, and hair that has maintained its growth phase by estrogen enters a resting state at a stretch by parturition and hair loss increases. Disease is included in postpartum alopecia.
- a subject means any individual organism, preferably a vertebrate, more preferably a mammal, and even more preferably a rodent such as a mouse, rat, gerbil, guinea pig, cat, puma, tiger, etc.
- rodent such as a mouse, rat, gerbil, guinea pig, cat, puma, tiger, etc.
- deer animals such as felines, deer and elk, rabbits, dogs, minks, sheep, goats, cows, horses, monkeys and humans, most preferably humans.
- the natriuretic peptide is selected from A-type natriuretic peptide (ANP), B-type natriuretic peptide (BNP), C-type natriuretic peptide (CNP), derivatives of these NPs, and these NPs 2 or more NP chimeric peptides or derivatives of the above NP chimeric peptides, and are not particularly limited as long as they have ANP activity, BNP activity or CNP activity. Particularly preferred is ANP, BNP or CNP.
- ANP is ANP-28 ( ⁇ -ANP) consisting of 28 amino acids, ⁇ -ANP [4-28] from amino acids 4 to 28 of ANP-28, and amino acids 5 to 28 of ANP-28.
- the ANP derivative has an amidated C-terminal of ANP, a methoxylated ANP C-terminal, a polyethylene glycol added to ANP, and a sugar chain added to ANP , ANP to which an alkyl chain is added, and ANP to which a fatty acid is added are included.
- the ANP may be ⁇ -ANP having a structure in which ANP-28 is an antiparallel dimer, or a high molecular weight ⁇ -ANP having a molecular weight of 13,000 obtained by cleaving the signal peptide from the ANP precursor. Particularly preferred is ⁇ -ANP or a derivative thereof.
- the amino acid sequence of human ANP-28 is shown as the sequence of SEQ ID NO: 1 in this specification.
- An ANP derivative preferably has 1 to 5, more preferably 1 to 3, more preferably 1 or 2 amino acids deleted or substituted or added in the amino acid sequence of ANP-28 and has ANP activity. Or a sequence having a homology of 85% or more, preferably 90% or more, more preferably 95% or more with the amino acid sequence of ANP-28, and having ANP activity.
- the ANP derivative has an amidated C-terminal of ANP, a methoxylated ANP C-terminal, a polyethylene glycol added to ANP, and a sugar chain added to ANP , ANP to which an alkyl chain is added, and ANP to which a fatty acid is added are included.
- any known ANP can be used on the condition that it has ANP activity.
- 819 ANP derivatives disclosed as AP1-AP819 in US Pat. No. 5,047,397 or US Pat. No. 4,804,650 32 ANP derivatives disclosed as Compound Nos. 1-32 in Tables 1-3 of US Pat. No. 5,204,328 There may be.
- ANP activity can be easily confirmed by known means, for example, by testing cGMP production activity in NPR-A receptor-expressing cells.
- ANP As the active ingredient of the present invention, either ANP or a derivative thereof can be used, but ANP-28 is preferred from the viewpoint of drug efficacy and availability.
- the ANP of the present invention can be produced by chemical synthesis or genetic manipulation using a human ANP gene (for example, Nature. 1984 312 (5990), pages 152-155), but ANP has already been marketed. Therefore, it can also be obtained from the market. Further, for example, it can be obtained as ANP (Human, 1-28) from Peptide Institute, Inc. (PEPTIDE INSTITUTE, INC).
- ANP that can be used in the present invention includes purified ANP from nature, recombinant ANP produced by a known genetic engineering technique, known chemical synthesis methods (for example, solid phase synthesis using a peptide synthesizer) ANP manufactured by the above method).
- Basic techniques such as gene recombination techniques, site-directed mutagenesis, and PCR techniques are known or well-known, and are described in, for example, Current-Protocols-In-Molecular-Biology; John Wiley & Sons (1998).
- BNP means 26 BNP-26, 32 BNP-32, 45 BNP-45 or derivatives thereof, respectively, as long as the amino acid has BNP activity, and is not particularly limited.
- the BNP may be a high molecular weight ⁇ -BNP having a molecular weight of about 13,000, in which a signal peptide is cleaved from a BNP precursor. Particularly preferred is BNP-32 or a derivative thereof.
- the amino acid sequence of human BNP-32 is shown as the sequence of SEQ ID NO: 41 in the present specification.
- the amino acid sequence of human BNP-26 is shown as the sequence of SEQ ID NO: 82 in the present specification.
- the BNP derivative preferably has 1 to 5, more preferably 1 to 3, more preferably 1 or 2 amino acids in the amino acid sequence of BNP-26, BNP-32 or BNP-45. And having a BNP activity, or having a homology of 85% or more, preferably 90% or more, more preferably 95% or more with the amino acid sequence of BNP-26, BNP-32 or BNP-45 And having BNP activity.
- BNP derivative has BNP C-terminal amidated, BNP C-terminal methoxylated, BNP polyethylene glycol added, BNP sugar chain added , BNP to which an alkyl chain is added, and BNP to which a fatty acid is added are included.
- any known BNP can be used on the condition that it has BNP activity.
- BNP derivatives disclosed in JP-T-2007-525213, 29 BNP derivatives disclosed as SEQ ID NOS: 1 to 29 in US Pat. No. 6028055, and the general formula of claim 1 of US Pat. No. 5,114,923 are disclosed.
- BNP activity can be easily confirmed by known means, for example, by testing cGMP production activity in NPR-A receptor-expressing cells.
- any of BNP-26, BNP-32, BNP-45 or derivatives thereof can be used, but BNP-32 is preferred from the viewpoint of medicinal efficacy and availability.
- the BNP of the present invention can be prepared by chemical synthesis or genetic manipulation using a human BNP gene (for example, JP-A-5-207891, JP-T2007-525957, JP-T2007-525213). No.) and BNP are already on the market and can be obtained from the market. Also, for example, it can be obtained as BNP-32 (human) from Peptide Institute, Inc. (PEPTIDE INSTITUTE, INC.).
- BNP that can be used in the present invention includes purified BNP from nature, recombinant BNP produced by a known genetic engineering technique, known chemical synthesis methods (for example, solid phase synthesis using a peptide synthesizer) BNP produced by the above method).
- Basic techniques such as gene recombination techniques, site-directed mutagenesis methods, PCR techniques and the like are known or well known, and are described in, for example, Current-Protocols-In-Molecular-Biology; John Wiley & Sons (1998), Japanese Patent Application Laid-Open No. 5-207789 Yes.
- CNP means 22 CNP-22 amino acids, 53 CNP-53 amino acids with 31 amino acid residues added to the N-terminus thereof, or derivatives thereof, and is particularly limited as long as it has CNP activity is not. Particularly preferred is CNP-22 or a derivative thereof.
- the CNP derivative preferably has 1 to 5, more preferably 1 to 3, more preferably 1 or 2 amino acids deleted, substituted or added in the amino acid sequence of CNP-22 or CNP-53, and Those having CNP activity, or having a homology of 85% or more, preferably 90% or more, more preferably 95% or more with the amino acid sequence of CNP-22 or CNP-53, and having BNP activity Means.
- CNP derivatives have CNP activity, CNP C-terminal amidated, CNP C-terminal methoxylated, CNP polyethylene glycol added, CNP sugar chain added , CNP added with an alkyl chain, and CNP added with a fatty acid.
- the amino acid sequence of human CNP-22 is shown as the sequence of SEQ ID NO: 81 in the present specification.
- the amino acid sequence of human CNP-53 is shown as the sequence of SEQ ID NO: 83 in the present specification.
- any known CNP can be used on the condition that it has CNP activity.
- a CNP derivative disclosed in JP-A-6-9688, a CNP derivative disclosed as VNP (SEQ ID NO: 4) and a peptide of SEQ ID NO: 9 in US Pat. No. 5,583,108 or a CD-NP disclosed in US Pat. No. 6,818,619 There may be.
- the presence or absence of CNP activity can be easily confirmed by known means. For example, the inhibitory effect on clot smooth muscle cell proliferation or cGMP production activity in NPR-B receptor-expressing cells can be tested. This can be confirmed.
- CNP-22 As the active ingredient of the present invention, any of CNP-22, CNP-53 or derivatives thereof can be used, but CNP-22 having a lower molecular weight is preferable from the viewpoint of absorbability.
- CNP-22 can be prepared by chemical synthesis or genetic manipulation using a human CNP gene, and is obtained as, for example, CNP-22 (human) from PEPTIDE INSTITUTE, INC. be able to.
- CNP that can be used in the present invention is produced by purified CNP from nature, genetically modified CNP produced by a known genetic engineering technique, or a known chemical synthesis method (for example, solid phase synthesis using a peptide synthesizer).
- Basic techniques such as gene recombination techniques, site-directed mutagenesis methods, PCR techniques and the like are known or well-known, and are described in, for example, Current-Protocols-In-Molecular-Biology; John Wiley & Sons (1998), Japanese Patent Laid-Open No. Hei 5-207789, etc. Yes.
- the origin of the natriuretic peptide is not particularly limited as long as it has CNP activity, BNP activity or ANP activity, but preferably NP derived from mammals or birds including humans, more preferably humans, monkeys, mice NP derived from rat or pig, particularly preferably NP derived from human.
- Conservative amino acid substitution is desirable for the amino acid that can be substituted in the ANP derivative, BNP derivative, and CNP derivative.
- Conservative amino acids are classified according to polarity and charge type. For example, glycine, alanine, valine, leucine, isoleucine, proline, etc. for nonpolar uncharged amino acids, phenylalanine, tyrosine, tryptophan for aromatic amino acids, serine, threonine, cysteine, methionine for polar uncharged amino acids
- Negatively charged amino acids such as asparagine and glutamine include aspartic acid and glutamic acid, and positively charged amino acids include lysine, arginine and histidine, respectively.
- proline when substituting proline with another nonpolar uncharged amino acid, or when substituting a nonpolar noncharged amino acid other than proline with proline, proline is not a three-dimensionally flexible structure. It is necessary to pay attention to.
- cysteine when cysteine is replaced with another polar uncharged amino acid, or when a polar other than cysteine is replaced with cysteine, cysteine can form a disulfide bond with other cysteine. It is necessary to pay attention to.
- natriuretic peptide (NP) in the present specification includes a chimeric peptide of two or more natriuretic peptides (NP) selected from ANP, BNP or CNP. That is, in the present specification, in the case of NP, A natriuretic peptide (NP) is a chimeric peptide of two or more natriuretic peptides (NP) selected from ANP, BNP or CNP, wherein a cyclic structure is formed by an intramolecular disulfide bond, The CNP, CNP-22, CNP-53, a peptide comprising any continuous amino acid sequence of 5 amino acids or more in the amino acid sequence of CNP-22 from which any 1 to 5 amino acids are deleted, substituted or added, Or a peptide selected from the group consisting of peptides comprising any continuous amino acid sequence of 5 or more amino acids in the amino acid sequence of CNP-53 in which 1 to 5 arbitrary amino acids have been deleted, substituted
- Peptide containing an amino acid sequence peptide containing any sequence of 5 amino acids or more in the amino acid sequence of BNP-32 from which any one to five amino acids have been deleted, substituted or added, one to five arbitrary A peptide selected from the group consisting of peptides comprising any continuous amino acid sequence of 5 amino acids or more in the amino acid sequence of BNP-45 in which the amino acid is deleted, substituted or added,
- the ANP is a peptide comprising ANP-28 or any continuous amino acid sequence of 5 or more amino acids in the amino acid sequence of ANP in which any 1 to 5 amino acids are deleted, substituted or added; It also means a chimeric peptide having CNP activity, BNP activity or ANP activity, or a derivative thereof.
- a more preferred chimeric peptide of natriuretic peptide (NP) in the present invention is a chimeric peptide of CNP and BNP. That is, Natriuretic peptide (NP) is a chimeric peptide of CNP and BNP that forms a cyclic structure by intramolecular disulfide bonds, The CNP, CNP-22, CNP-53, a peptide comprising any continuous amino acid sequence of 5 amino acids or more in the amino acid sequence of CNP-22 from which any 1 to 5 amino acids are deleted, substituted or added, Or a peptide selected from the group consisting of peptides comprising any continuous amino acid sequence of 5 or more amino acids in the amino acid sequence of CNP-53 in which 1 to 5 arbitrary amino acids have been deleted, substituted or added,
- the BNP is BNP-26, BNP-32, BNP-45, or any arbitrary sequence of 5 amino acids or more in the amino acid sequence of BNP-26 from which any one to 5 amino acids have
- Peptide containing an amino acid sequence peptide containing any sequence of 5 amino acids or more in the amino acid sequence of BNP-32 from which any one to five amino acids have been deleted, substituted or added, one to five arbitrary
- CNP or BNP means a CNP-BNP chimeric peptide in addition to the meaning of either CNP or BNP.
- CNP-22 and CNP-53 is not particularly limited as long as it has CNP activity, but preferably CNP derived from mammals or birds including humans, more preferably human, monkey, mouse CNP derived from rat or pig, particularly preferably CNP derived from human.
- origin of BNP-26, BNP-32, and BNP-45 is not particularly limited as long as it has BNP activity, but it is preferably BNP derived from mammals or birds including humans, more preferably Is BNP derived from human, monkey, mouse, rat or pig, particularly preferably BNP derived from human.
- ANP-28 is not particularly limited as long as it has ANP activity, but preferably ANP derived from mammals or birds including humans, more preferably humans, monkeys, mice, rats. Or it is an ANP derived from a pig, particularly preferably an ANP derived from a human.
- the derivative of two or more NP chimeric peptides selected from ANP, BNP, or CNP is preferably 1 to 5, more preferably 1 to 3, more preferably in the amino acid sequence of these NP chimeric peptides. It means that one or two amino acids are deleted, substituted or added and have CNP activity or BNP activity.
- the amino acid that can be substituted in the derivative of the chimeric peptide of the natriuretic peptide (NP) derivative is the same as the amino acid that can be substituted for the ANP derivative, BNP derivative, and CNP derivative.
- the derivative of the natriuretic peptide (NP) derivative chimera peptide is an amidated C-terminal of the NP chimeric peptide, C-terminal of the NP chimeric peptide Is obtained by adding polyethylene glycol to NP chimeric peptide, sugar chain added to NP chimeric peptide, alkyl chain added to NP chimeric peptide, and NP chimeric peptide The thing added with the fatty acid is also included.
- the amino acid sequence of the human ANP peptide represented by SEQ ID NO: 1, the amino acid sequence of the human BNP peptide represented by SEQ ID NO: 41, and the amino acid sequence of the human CNP peptide represented by SEQ ID NO: 81 are as shown in FIG. And four different sequences separated by three common sequences represented by amino acid sequences of “CFG”, “DRI”, and “SGLGC”, respectively. Therefore, as a chimeric peptide of two or more NPs selected from ANP, BNP or CNP, at least 78 kinds of SEQ ID NOs: 2 to 40 and SEQ ID NOs: 42 to 80 represented by combinations of these four different sequences are used. Chimeric peptides are exemplified. These chimeric peptides and derivatives thereof are considered to have properties common to ANP, BNP and CNP. That is, these chimeric peptides and derivatives thereof can be used as active ingredients of the therapeutic agent for alopecia of the present invention.
- any known natriuretic peptide (NP) chimeric peptide or its derivative can be used on the condition that it has ANP activity, BNP activity or CNP activity.
- NP natriuretic peptide
- ANP activity BNP activity or CNP activity
- BNP activity BNP activity or CNP activity
- CNP activity can be easily confirmed by known means, for example, to test cGMP production activity in NPR-A receptor-expressing cells or NPR-B-expressing cells. Can be confirmed.
- ANP, BNP, CNP, derivatives of these NPs, or two or more NP chimeric peptides selected from these NPs are known and can be prepared by chemical synthesis or genetic manipulation.
- the disease to which the therapeutic agent for alopecia of the present invention is applied is not particularly limited as long as it is so-called alopecia in which the hair becomes thin or falls off.
- the therapeutic agent for alopecia of the present invention can be applied to various types of alopecia.
- alopecia to which the therapeutic agent for alopecia of the present invention can be applied examples include alopecia areata, male pattern alopecia, postpartum alopecia, female pattern alopecia, seborrheic alopecia, critical alopecia, senile Alopecia is preferable, and alopecia areata, male pattern alopecia, postpartum alopecia, and female pattern alopecia are particularly preferable from the viewpoint of the healing effect, and alopecia areata is particularly preferable.
- the male pattern baldness may be either male male pattern baldness or female male pattern baldness.
- alopecia areata it can be any of the following: normal alopecia areata, multiple alopecia areata, general alopecia, general alopecia, general alopecia, serpentine alopecia May be any of S1 to S5 or B0 to B2.
- the therapeutic agent for alopecia of the present invention is extremely effective and safe as a therapeutic agent for refractory tortuous alopecia that is difficult to cure or long-term remission.
- the therapeutic agent for alopecia of the present invention comprises A-type natriuretic peptide (ANP), B-type natriuretic peptide (BNP), C-type natriuretic peptide (CNP), derivatives of these natriuretic peptides (NP), these NPs 2 or more NP chimeric peptides selected from the above or a derivative of two or more NP chimeric peptides selected from these NPs as the active ingredient, and the administration route and dosage form are not particularly limited .
- the therapeutic agent for alopecia of the present invention includes ANP, BNP, CNP, derivatives of these NPs, two or more NP chimeric peptides selected from these NPs or derivatives thereof, steroid agents, antihistamines, vasodilators Agent, male hormone activity inhibitor, female hormone agent, antibiotic, antifungal agent, pentadecane, cytopurine (6-benzylaminopurine), t-flavanone, adenosine, cephalanthin, glycyrrhizin, a combination of glycyrrhizin, methionine and glycine (Registered trademark), Cyclosporin A, Keishikari Kyokubo oyster hot water, Hankasa Kobokuto, biotin, anthralin, tricyclic antidepressant may be included as a mixture, or may be used in combination .
- betamethasone dexamethasone, clobetasol, prednisolone, mometasone, methylprednisolone, deprodon, difluprednate, fluocinonide, amsinonide, triamcinolone, difluprednate, hydrocortisone are preferable, and betamethasone or clobetasol is particularly preferable.
- antihistamine azelastine, oxatomide, fexofenadine, emedastine, ebastine, cetirizine, bepotastine, olopatadine, and loratadine are preferable.
- vasodilator minoxidil and carpronium chloride are preferable.
- male hormone activity inhibitor finasteride is preferable.
- estrogen estradiol or progesterone is preferable.
- antibiotic gentamicin is preferred.
- antifungal agent amphotericin B, nystatin, ketoconazole, terbinafine, flucytosine, fluconazole, itraconazole, griseofulvin, and micafungin are preferable.
- the therapeutic agent for alopecia of the present invention can be formulated using a widely used technique.
- As the preparation form an external preparation can be exemplified.
- the preferred dosage form of the therapeutic agent for alopecia of the present invention is an external preparation (percutaneous absorption agent) such as a gel, an ointment or a liquid.
- the external preparation is not particularly limited as long as it can be directly applied, sprayed, or affixed to a required site (affected area) of the skin.
- the form of the therapeutic agent for alopecia of the present invention is preferably an ointment, gel, cream, lotion, liquid, spray, gel spray, foam, patch, shampoo, treatment, scalp treatment From the viewpoint of ease of application, ointments, gels, creams, and liquids are more preferable, and gels, ointments, and liquids are more preferable.
- NP natriuretic peptide
- the gel agent may be any of a water-containing gel, an anhydrous gel, or a low water content gel made of a swellable gel-forming material. Further, it may be either a hydrogel base or a liogel base, but is preferably a transparent hydrogel based on an inorganic or organic polymer. As with formulations containing oils and fats, the gel itself is not absorbed by the skin.
- the hydrogel base is non-fat and has a consistency like an ointment, and aims to increase the transdermal absorbability of the drug.
- the liogel base is made by suspending stearyl alcohol or the like in propylene glycol. It is gelled and has excellent transdermal absorbability and hygroscopicity. The gel may be used as a gel spray by filling a spray container.
- the gel agent of the present invention is an active ingredient in a hydrophilic gel base containing carboxyl vinyl polymer, sodium polyacrylate, sodium polyacrylate, (vinyl methyl ether / ethyl maleate) copolymer, polymethacrylate, propylene glycol and the like. It may be a gel agent in which natriuretic peptide (NP) is uniformly dispersed.
- NP natriuretic peptide
- examples of such gel agents include, for example, commercially available sustained water retention products such as Lubragel NP, Lubragel CG, Lubragel DV, Lubragel MS, Lubragel OIL, Lubragel TW, Lubragel DS, etc., which are commercially available products of ISP Japan. Gels uniformly dispersed in the agent are included.
- gel agent of the present invention is a gel preparation prepared according to Example 2.
- the liquid preparation of the present invention is a solution in which natriuretic peptide (NP) as an active ingredient is dissolved in alcohol, propylene glycol, polyethylene glycol, water or the like as a base, preferably natriuretic peptide is dissolved in physiological saline. It is the liquid agent which consists of an aqueous solution.
- the aqueous solution may contain a small amount of an organic base such as alcohol, propylene glycol and polyethylene glycol in addition to physiological saline.
- natriuretic peptide as an active ingredient, butyric acid, lactic acid, phosphoric acid, glycine, citric acid, hydrochloric acid, propionic acid,
- One or two or more of the group consisting of butyric acid, benzoic acid or their salts are combined to form an acidic solution, or alcohols and / or N-methyl-2-pyrrolidine, dimethylformamide, dimethyl sulfoxide, methylparaben
- One or a combination of two or more can be used as a polar organic liquid, and the pH can be adjusted to 3.0 to 7.0.
- the ointment preparation of the present invention may be either an oleaginous base or a water-soluble base, and both can be easily obtained according to known methods.
- Oily bases such as petrolatum are less irritating and odorless, and are excellent in skin protection, softening, crust removal, granulation, and epithelialization.
- the water-soluble base is an ointment mainly composed of a macrogol base, and has a strong action of absorbing and removing aqueous secretions.
- ointment of the present invention is an ointment prepared according to Example 2.
- the cream (emulsion base) may be an oil-in-water base (O / W) (burnishing cream) or a water-in-oil base (W / O) (cold cream).
- Oil-in-water bases have the advantage that the oil-soluble component is less than the water-soluble component, and the whiteness of the cream appears to disappear when applied. It stretches well, has a good feeling on sweaty skin and is cosmetically superior. In addition, since it is excellent in absorbability into the skin, it is a good indication for chronic hypertrophic lesions.
- Water-in-oil bases are sometimes called cold creams because they have less water-soluble components than oil-soluble components and have a cooling effect when applied to the skin.
- the lotion means a liquid external preparation in which natriuretic peptide is dissolved or evenly dispersed in the liquid.
- a lotion is suitable for use in the hair portion or the like.
- the form of the lotion may be any of a suspension lotion base, an emulsion lotion, and a solution lotion base.
- the patch agent promotes the absorption of the drug by attaching a component containing a natriuretic peptide to the patch and utilizing the airtightness of the patch. By applying a patch, scratching can be prevented.
- the spray agent is a solution in which a natriuretic peptide is made into a solution and sprayed by gas pressure or manual operation. This is convenient when used over a wide range.
- the foam agent is a spray agent that is released in the form of foam when a natriuretic peptide is made into a solution and a surfactant is contained.
- the foam is excellent in that the scalp has good adhesion.
- a shampoo is a dosage form in which a natriuretic peptide can be mixed or dissolved in a shampoo and a drug applied simultaneously with shampooing. Since shampoo is a surfactant, it has the effect of penetrating natriuretic peptide into the scalp. In particular, in seborrheic alopecia, a shampoo is advantageous because it can also remove excess sebum.
- the treatment agent is a dosage form in which a natriuretic peptide is mixed or dissolved in a treatment agent used for shampooing, and a drug can be applied simultaneously with the treatment.
- the treatment agent can supplement the scalp with moisture and oil at the same time as the drug is applied.
- a treatment agent is advantageous because it can serve both as moisturizing the scalp and replenishing oil simultaneously with the application of the drug.
- “Scalp treatment agent” refers to a treatment agent that specifically contains ingredients intended to moisturize and replenish the scalp.
- scalp treatment agents are blended with various plant extract components such as persimmon rosemary extract, mukuroji extract, and palm extract.
- Tonic preparations together with natriuretic peptides, are 50% to 70% alcohol and water as a base material, hinokitiol, panthenol, an ingredient that keeps the scalp healthy such as panthenol and sembly extract, glycyrrhizic acid that has a female hormone-like action
- a moisturizing component such as a bactericidal agent, glycerin, salicylic acid that makes it easy to remove dandruff, menthol that prevents itching, and a refreshing feeling.
- Tonic preparations are used after washing the hair to prevent dandruff and head odor, keep the hair clean, prevent itching and stuffiness, and eliminate discomfort related to hair. It is advantageous as a dosage form of a therapeutic agent for alopecia that often accompanies.
- the therapeutic agent for alopecia of the present invention is a transdermal external preparation comprising an appropriate amount of natriuretic peptide, various bases, and additives as necessary.
- natriuretic peptide which is an active ingredient applied to the skin surface, can reach and maintain an effective concentration in the lesion. Therefore, a dosage form and a base may be appropriately selected according to symptoms and patients.
- additives can be used as appropriate according to the purpose.
- the following can be used as an additive.
- Vaseline Can be used as a base for ointment preparations. It is one of the safest bases, although its viscosity and consistency change with temperature and the hardness differs in winter and summer. There are yellow petrolatum and highly pure white petrolatum, but any use is possible.
- Propylene glycol Can be used as a drug solvent, a solubilizing agent, or a base.
- Paraffin can be used to adjust the consistency of the ointment. Since emulsification is relatively easy, it may be used as an oily agent for cream production.
- Honey beeswax processed beeswax wax, blended with vegetable oils and fats, can also be used as a “Japan bureau” simple ointment.
- White beeswax is a beeswax that has been bleached to improve color and odor.
- Macrogol A mixture of polyethylene glycols with different molecular weights. It has excellent drug solubility and mixing properties, and absorbs water well, so it is suitable for adsorbing and removing the eluate from mucous membranes and affected areas.
- Stearyl alcohol Can be used as an emulsion lotion.
- Isopropanol Can be used as a solvent or a solubilizing agent.
- Benzyl alcohol Can be used as a solubilizer, preservative, etc.
- Paraoxybenzoates Can be used as preservatives, preservatives, and stabilizers.
- Gelled hydrocarbon Generally called “plasty base”, liquid paraffin is gelled (semi-solid) with polyethylene.
- Citric acid, sodium citrate Can be used as a buffering agent or pH adjuster.
- Squalene used as a base, slightly oily and less sticky than liquid paraffin. It can be widely used in emulsion lotions as well as creams.
- Lanolins Fats and oils obtained from sheep's hair, which have difficulties in color and odor, but are useful for improving skin flexibility.
- Glycerin As a moisturizer, it can be blended in creams and the like.
- Polyoxyethylene hydrogenated castor oil Can be used as an emulsifier, a solubilizer and the like.
- Sorbitan fatty acid ester, glycerin fatty acid ester Can be used as an emulsifier.
- the therapeutic agent for alopecia of the present invention may further contain a moisturizing agent (emollient), a symptom alleviating agent, etc. as described below.
- a moisturizing agent emollient
- a symptom alleviating agent etc. as described below.
- Moisturizer emollient: A moisturizer provides moisture and oil to the skin. Moisturizers are most effective when the skin is already moistened, such as immediately after bathing or showering.
- the components contained in the humectant are glycerin, mineral oil, petrolatum and the like. There are lotions, creams, ointments, bath oils, etc. as humectants. Those containing urea, lactic acid, or glycolic acid have an excellent moisturizing effect.
- Symptom relieving drugs Many skin diseases are accompanied by itching. Itching and mild pain can be reduced by blending sedatives, specifically chamomile, eucalyptus, camphor, menthol, zinc oxide, talc, glycerin, calamine and the like. In order to suppress itching due to allergy, an antihistamine such as diphenhydramine may be contained.
- various bases moisturizers, ultraviolet absorbers, alcohols, chelates, pH adjusters, preservatives, thickeners, colorants, Fragrance, filler, excipient, disintegrant, bulking agent, binder, film agent, solubilizer, suspending agent, buffer, stabilizer, preservative, surfactant, antioxidant, dispersant , Emulsifiers, solubilizers, solubilizers and the like can be combined in any combination.
- various drugs such as analgesic / antibacterial agents, bactericides / disinfectants, vitamins, skin softeners, and the like may be added as necessary.
- the skin external preparation composition of the present invention When used as a skin quality improving agent, it can be used as a skin care cosmetic or quasi-drug.
- Specific usage forms include creams, foams, Mention may be made of lotions, packs, skin softeners, emulsions, foundations, makeup bases, essences, soaps, liquid detergents, bath preparations, sun creams, sun oils or spray type liquids. Any of them can be easily produced by applying well-known or Kochi formulation techniques.
- the gel is obtained by dissolving an appropriate amount of natriuretic peptide in distilled water or physiological saline to form an aqueous solution according to a known or well-known method, and further mixing this with a known or well-known gel base and stirring. be able to.
- the effect is not sufficient when the concentration of natriuretic peptide is 1 ⁇ g / g or less, and a sufficient effect can be obtained even if the concentration is not more than 1000 ⁇ g / g.
- the final natriuretic peptide concentration in the gel is 1-1000 ⁇ g / g, more preferably 10-500 ⁇ g / g, even more preferably 20-300 ⁇ g / g, still more preferably 30-200 ⁇ g / g, particularly preferably 50. It is preferable to prepare so as to be ⁇ 100 ⁇ g / g.
- Examples of the gel base composed of a polymer inorganic component include water-containing or water-absorbing silicates such as aluminum silicate such as bentonite, magnesium silicate-aluminum, or colloidal silica. Natural, semi-synthetic or synthetic polymers can be used as the gel base made of a macromolecular organic substance.
- Natural and semi-synthetic polymers include, for example, polysaccharides such as cellulose, starch, tragacanth, gum arabic, xanthan gum, agar, gelatin, alginic acid and its salts such as sodium alginate and its derivatives, lower alkyl cellulose such as methylcellulose or ethylcellulose Carboxy- or hydroxy-lower-alkyl celluloses such as carboxymethyl cellulose or hydroxypropyl cellulose.
- the synthetic gel base include polyvinyl alcohol, polyvinyl pyrrolidone, polyacrylic acid, and mepolytacrylic acid.
- gel base dispersed uniformly in commercially available continuous water retention agents such as Lubragel NP, Lubragel CG, Lubragel DV, Lubragel MS, Lubragel OIL, Lubragel TW, Lubragel DS, etc., which are commercially available products of ISP Japan.
- An agent can also be used.
- These gel bases may be one kind or a mixture of two or more kinds of gel bases.
- the ointment (Vaseline preparation) is prepared by dissolving an appropriate amount of natriuretic peptide in distilled water or physiological saline to form an aqueous solution according to a known or well-known method, and further mixing this with a known or well-known petrolatum and stirring. Can be obtained.
- the effect is not sufficient when the concentration of natriuretic peptide is 1 ⁇ g / g or less, and a sufficient effect can be obtained even if the concentration is not more than 1000 ⁇ g / g.
- the final natriuretic peptide concentration in the ointment is 1-1000 ⁇ g / g, more preferably 10-500 ⁇ g / g, even more preferably 20-300 ⁇ g / g, still more preferably 30-200 ⁇ g / g, particularly preferably 50. It is preferable to prepare so as to be ⁇ 100 ⁇ g / g.
- the liquid preparation is, for example, 0.01 mg to 10 mg of human ANP (1-28) (manufactured by Peptide Laboratories), human BNP-32 (manufactured by Peptide Laboratories) or human CNP-22 (Co., Ltd.) as the main agent.
- Peptide Laboratories can be dissolved in 10 ml of physiological saline to prepare solutions each having a natriuretic peptide concentration of 1-1000 ⁇ g / g. Since the specific gravity of water is 1, the ANP concentration, BNP concentration or CNP concentration in this case is 1 to 1000 ⁇ g / g by weight.
- the effect is not sufficient when the concentration of natriuretic peptide is 1 ⁇ g / g or less, and a sufficient effect can be obtained even if the concentration is not more than 1000 ⁇ g / g.
- the preferable concentration of the aqueous solution preparation of natriuretic peptide is 1-1000 ⁇ g / g, more preferably 10-500 ⁇ g / g, still more preferably 20-300 ⁇ g / g, still more preferably 30-200 ⁇ g / g, particularly preferably 50-100 ⁇ g / g. g.
- transdermal absorption aid examples include acetic acid, sodium acetate, limonene, menthol, salicylic acid, hyaluronic acid, oleic acid, N, N-diethyl-m-toluamide, n-butyl stearate, benzyl alcohol, isopropyl myristate, Examples include isopropyl palmitate, polypropylene glycol, crotamiton, diethyl sebacate, N-methylpyrrolidone, N-ethylpyrrolidone, lauryl alcohol and the like.
- antiseptics and antioxidants may be added as desired.
- the concentration of natriuretic peptide in the therapeutic agent for alopecia can be appropriately selected in consideration of symptoms, age, dosage form and the like.
- the concentration of natriuretic peptide is preferably 1 to 1000 ⁇ g / g, more preferably 10 to 500 ⁇ g / g, still more preferably 20 to 300 ⁇ g / g, for external preparations such as liquids, gels, ointments and lotions.
- the amount is preferably 30 to 200 ⁇ g / g, particularly preferably 50 to 100 ⁇ g / g. For younger patients and patients with weak skin, it is preferable to use those having a concentration of 20 to 100 ⁇ g / g.
- the specific gravity of the solution used in the liquid preparation of the present invention is approximately 1, when the concentration of ANP, BNP or CNP is expressed in units of ⁇ g / g in the liquid preparation, sodium in units of ⁇ g / ml is used. This has the same meaning as the concentration of diuretic peptide.
- this alopecia treatment agent varies depending on symptoms, age, dosage form, etc., but it is typically twice a day and the administration period is 7 to 28 days.
- administration period is 7 to 28 days.
- For chronic alopecia with fixed symptoms it is desirable to administer for about 28 days, but for the acute phase, administration for about 7 days is sufficient.
- administration for 14 days or more is desirable for adults, but administration for about 7 days is sufficient for minors.
- Example 1 Subject diagnosis and evaluation. First, subjects were diagnosed and evaluated prior to administration of the natriuretic peptide preparation. The diagnosis and evaluation methods for the subjects are as follows.
- Diagnosis of the subject The subject is a patient with alopecia areata, male pattern alopecia, postpartum alopecia, female pattern alopecia, critical alopecia or senile alopecia. Diagnosis and treatment of these subjects were performed by the inventor as doctors.
- the left and right painting method is suitable.
- the left-right coating method is, for example, a method of applying an external medicine containing an active ingredient to be tested on the left side of a diseased site and applying an external medicine containing no active ingredient on the right side to confirm the therapeutic effect. It is.
- the test of the preparation of the present invention was also conducted according to the left and right coating method in the preliminary test. However, in view of medical ethics, the preliminary test by the left and right coating method was kept to a minimum, and when the preliminary test was not performed, the therapeutic effect was determined by comparing before and after application.
- the preparation of a gel containing NP as an active ingredient includes human ANP (1-28) (manufactured by Peptide Laboratories), human BNP-32 (manufactured by Peptide Laboratories), and human CNP-22 (manufactured by Co., Ltd.).
- 1 mg of each NP solution having a concentration of 1000 ⁇ g / ml obtained by weighing 3 mg of any of Peptide Laboratories and dissolving it in 3 ml of purified water is uniformly distributed in 9 g of Lubragel NP (IS Japan) The mixture was stirred and mixed to prepare an ANP gel, BNP gel and CNP gel having a concentration of 100 ⁇ g / g.
- each NP solution having a concentration of 1000 ⁇ g / ml obtained above is diluted with 500 ⁇ l of physiological saline to prepare a concentration of 500 ⁇ g / ml, and 1 ml of this solution is 9 g of rubragel NP (IS Japan Co., Ltd.).
- the mixture was stirred and mixed uniformly to prepare ANP gel, BNP gel and CNP gel having a concentration of 50 ⁇ g / g.
- ANP ointment was uniformly mixed with 9 g of Japanese petrolatum white petrolatum with high-speed stirring, and stirred to prepare ANP ointment, BNP ointment and CNP ointment at a concentration of 100 ⁇ g / g.
- each NP solution with a concentration of 1000 ⁇ g / ml obtained above is diluted with 500 ⁇ l of physiological saline to prepare a concentration of 500 ⁇ g / ml, and 1 ml of this solution is stirred into 9 g of Japanese Pharmacopoeia white petrolatum at high speed.
- ANP ointment, BNP ointment and CNP ointment with a concentration of 50 ⁇ g / g were prepared by mixing uniformly and stirring.
- 300 ⁇ l of the BNP solution having a concentration of 1000 ⁇ g / ml obtained above is diluted with 700 ⁇ l of physiological saline to prepare a concentration of 300 ⁇ g / ml, and 1 ml of this solution is stirred into 9 g of Japanese Pharmacopoeia white petrolatum at high speed.
- a BNP ointment with a concentration of 30 ⁇ g / g was prepared by mixing uniformly and stirring.
- BNP betamethasone: gentamicin combination
- BNP, betamethasone and gentamicin combination were prepared by obtaining “Dermosol-G Lotion” manufactured by Iwaki Pharmaceutical Co., Ltd. in “1. Preparation of gel preparation”. It was prepared by mixing with an equal volume of the gel of BNP. In the present specification, this is called a BNP: betamethasone: gentamicin combination.
- Delmozole G lotion contains betamethasone valerate at a concentration of 1200 ⁇ g / ml and gentamicin sulfate at a concentration of 1000 ⁇ g / ml, so that CNP gel at a concentration of 100 ⁇ g / g and Delmozol G lotion are 1: 1.
- a mixture containing CNP at a concentration of 50 ⁇ g / g, betamethasone valerate at a concentration of 600 ⁇ g / ml, and gentamicin sulfate at a concentration of 500 ⁇ g / ml was prepared. In the present specification, this is referred to as a 50 ⁇ g / g BNP: 600 ⁇ g / ml betamethasone: 500 ⁇ g / ml gentamicin combination.
- CNP betamethasone: gentamicin combination
- Preparation of CNP, betamethasone and gentamicin combination was obtained by “Dermosol-G Lotion” manufactured by Iwaki Pharmaceutical Co., Ltd. in the above “1. Production of gel preparation”. It was prepared by mixing with an equal volume of CNP gel. In the present specification, this is called a CNP: betamethasone: gentamicin combination.
- Delmozole G lotion contains betamethasone valerate at a concentration of 1200 ⁇ g / ml and gentamicin sulfate at a concentration of 1000 ⁇ g / ml, so that CNP gel at a concentration of 100 ⁇ g / g and Delmozol G lotion are 1: 1.
- a mixture containing CNP at a concentration of 50 ⁇ g / g, betamethasone valerate at a concentration of 600 ⁇ g / ml, and gentamicin sulfate at a concentration of 500 ⁇ g / ml was prepared. In the present specification, this is referred to as a 50 ⁇ g / g CNP: 600 ⁇ g / ml betamethasone: 500 ⁇ g / ml gentamicin combination.
- CNP gel at a concentration of 50 ⁇ g / g and Delmosol G lotion at a volume ratio of 1: 1
- CNP at a concentration of 25 ⁇ g / g
- betamethasone valerate at a concentration of 600 ⁇ g / ml
- this is referred to as a 25 ⁇ g / g CNP: 600 ⁇ g / ml betamethasone: 500 ⁇ g / ml gentamicin combination.
- BNP clobetasol combination
- Delmobeto Scarplottion 0.05% contains clobetasol propionate at a concentration of 500 ⁇ g / g
- BNP gel at a concentration of 100 ⁇ g / ml and Delmobeto Scarpration 0.05% are mixed in a volume ratio of 1: 1.
- a mixture containing BNP at a concentration of 50 ⁇ g / ml and clobetasol propionate at a concentration of 250 ⁇ g / g was prepared. In the present specification, this is referred to as a 50 ⁇ g / ml BNP: 250 ⁇ g / g clobetasol combination.
- CNP clobetasol combination
- Delmobeto Scarplottion 0.05% contains clobetasol propionate at a concentration of 500 ⁇ g / g
- CNP gel at a concentration of 100 ⁇ g / ml and Delmobeto Scarpration 0.05% are mixed in a volume ratio of 1: 1.
- a mixture containing CNP at a concentration of 50 ⁇ g / ml and clobetasol propionate at a concentration of 250 ⁇ g / g was prepared. In the present specification, this is called a 50 ⁇ g / ml CNP: 250 ⁇ g / g clobetasol combination.
- CNP carpronium chloride mixture
- Preparation of a mixture of CNP and carpronium chloride was obtained by the above-mentioned "1.
- Preparation of gel preparation obtained from Calyoran (trademark) 5% (CALPRANIN) manufactured by Taiyo Pharmaceutical Co., Ltd. It was prepared by mixing with an equal volume of CNP gel. In the present specification, this is called a CNP: carpronium chloride combination. Since 5% calplanin solution contains carpronium chloride at a concentration of 50 mg / ml, 50 ⁇ g / ml was prepared by mixing CNP gel at a concentration of 100 ⁇ g / ml and 5% calplanin solution at a volume ratio of 1: 1.
- a mixture containing CNP at a concentration of 5 mg and carpronium chloride at a concentration of 50 mg / ml was prepared. In the present specification, this is referred to as a 50 ⁇ g / ml CNP gel: 50 mg / ml carpronium chloride mixture.
- Example 3 Subject Diagnosis and Treatment Prior to administration of the ANP gel, BNP gel, CNP gel, BNP ointment and CNP ointment of the present invention, as a routine in dermatological practice, sex, age, medical history, family history to the subject When allergies were suspected, a scratch test for major allergens and their evaluation were conducted.
- dermatological practice there are many patients with strong immunoreactivity to specific allergens and relatively allergic predispositions such as atopic dermatitis.
- conducting a family history and past medical history of allergic diseases and conducting a scratch test for major allergens are widely used as a simple auxiliary test.
- Therapeutic effect on alopecia areata: ANP: Table 1, Table 2 BNP: Table 3-1 and Table 3-2 CNP: Table 4, Table 5, Table 6, Table 7-1 BNP: betamethasone: gentamicin combination: Table 7-2 CNP: betamethasone: gentamicin combination: Table 7-3 Therapeutic effect on male pattern baldness: ANP: Table 8 BNP: Tables 9-1 and 9-2 CNP: Table 10-1, Table 10-2 CNP: betamethasone: gentamicin combinations: Table 10-3 CNP: clobetasol combinations: Table 10-4 CNP: carpronium chloride mixture: Table 10-5 Multi-layer application of CNP gel and minoxidil: Table 10-6 Multi-layer application of BNP gel and minoxidil: Table 10-7 Therapeutic effect on postpartum alopecia: ANP: Table 10-8 BNP: Table 10-9 CNP: Table 11-1 Therapeutic effect on female pattern alopecia: ANP: Table 10-8 BNP: Table 10-9 CNP: Table 11-1 Therapeutic effect on female pattern alopecia
- the non-relapse period refers to a period in which the symptoms did not relapse even after the treatment with the preparation of the present invention was interrupted after the symptoms were relieved.
- photographs before and after applying the NP preparation were recorded for all cases. Among them, photographs of some cases are shown in the figure.
- Example 4 Therapeutic effect of ANP gel on alopecia areata Table 1 (cases A1 to A5) and 2 (cases A6 to A7) show the therapeutic effects of ANP gel on alopecia areata.
- Case A1 The test subject was a 33-year-old woman, and the hair loss range was S3, and she was a patient with severe alopecia areata of B1 with eyebrow hair loss in addition to the head. There is a history of atopic dermatitis, and alopecia that appeared as atopic dermatitis worsened is also associated. The results of the scratch test were house dust 2+, mite 1+, camogaya 2+ and ragweed 2+. In this test subject, scalp-like scales and erythema accompanied by pruritus were found on the scalp at the hair loss site, and critic alopecia was complicated.
- Case A2 The test subject was a 33-year-old female and was a patient with severe alopecia areata having a hair loss range of S3.
- the results of the scratch test were house dust 2+, mite 3+, cedar 3+, duck 2+ and ragweed 2+.
- the subject was treated for 6 months with topical steroids, carpronium chloride, and cephalanthin. No changes were seen.
- FIG. 7 shows a photograph of the hair loss spots before application and a photograph of the hair loss spots after 100 ⁇ g / g ANP gel was applied twice a day for 5 weeks. In the case of this test subject, soft hair growth was observed, but no further hair growth occurred and no long hair was present.
- Case A3 The test subject was a 52-year-old female and was a patient with severe alopecia areata having a hair loss range of S3.
- the results of the scratch test were house dust 1+, cedar 2+, camouflage 1+, and ragweed 1+.
- This test subject continued night shift, and a bald patch appeared on the frontal region about a year ago, and then showed an expanding tendency, and a bald area appeared frequently on the entire scalp.
- Application of carpronium chloride to the bald patch was continued for 8 months. However, the range of hair loss was widened, but no therapeutic effect was observed.
- This subject is, erythema on the scalp of the hair loss part, crusts, inflammatory conditions of the scales and the like are the cases that can not be seen.
- this test subject is the same test subject as the test subject of case C15.
- Case A4 The test subject was a 32-year-old male and was a patient with alopecia areata having a hair loss range of S1. A history of atopic dermatitis and allergic rhinitis. The results of the scratch test were house dust 2+, mite 3+, cedar 2+, duck 2+ and ragweed 2+. This test subject was triggered by mental stress from one month ago, and a bald area appeared on the left side of the head, and then a bald area appeared on the top and right side of the head. Accompanied by pruritus.
- Case A5 The test subject was a 16-year-old male, and the hair loss range was S3. This test subject has atopic dermatitis. The results of the scratch test were house dust 3+, tick 3+, camogaya 2+ and ragweed 1+. The subject underwent adenoid and tonsillectomy operations at the age of 6 and developed alopecia areata from the age of 7 and showed hair loss on the eyebrows and lower limbs in addition to the head. This test subject did not heal even after steroid internal use or topical use. The scalp of this test subject's hair loss site was infiltrated with erythema and scales and was accompanied by pruritus. In addition, this test subject is the same test subject as the test subject of case B3.
- Case A6 The subject is a 50-year-old woman, hair loss range in S2, is alopecia areata patients with severe multiple alopecia.
- Her mother has a history of alopecia areata and her child has allergic rhinitis and chronic urticaria.
- the results of the scratch test were house dust 1+, tick 1+, camogaya 2+, and ragweed 1+.
- scalp-like scales and erythema accompanied by pruritus were found on the scalp at the hair loss site, and critic alopecia was complicated.
- the subject developed multiple alopecia areata 10 years ago and has repeated partial remission and relapse of alopecia areata. This test subject tends to exacerbate hair loss symptoms when he is busy. Topical steroids and carpronium chloride and oral antiallergic agents were not effective after 6 months.
- this test subject is the same test subject as the test subject of case C3 and case C4.
- a 100 ⁇ g / g ANP gel was applied to the multiple hair loss spots at the top of this subject for 2 weeks, but there was no effect, bulky scales increased, red spots appeared, itching, hair loss increased, hair loss The range has rather expanded (see FIG. 11).
- Case A7 The test subject was a 22-year-old female, and the hair loss range was S3, which is a severe patient with alopecia areata having a serpentine alopecia type that is said to be intractable.
- the subject has a history of atopic dermatitis and allergic rhinitis.
- the subject's grandfather has atopic dermatitis, and his father, mother, and brother have allergic rhinitis.
- the results of the scratch test were house dust 2+, mite 3+ and camogaya 1+. This test subject developed a hair loss spot more than a year and a half ago, and the hair loss spot was clearly stripped along the outer edge of the hair part without hair growth at all.
- Case B1 The test subject was a 63-year-old woman, and the hair loss range was S2, which is a severe patient with multiple alopecia areata.
- the subject had a history of allergic rhinitis and had atopic dermatitis.
- the results of the scratch test were house dust 2+, mite 1+, camogaya 2+, and ragweed 1+.
- This test subject's alopecia areata lasts more than a year and a half.
- the subject had previously applied steroids and carpronium chloride for 10 months to the bald area, but had no effect and no hair growth.
- this test subject is the same test subject as the test subject of case C12.
- Case B2 The test subject was a 13-year-old male with alopecia areata having a hair loss range of S1. No scratch test was performed on this subject.
- Case B3 The test subject was a 16-year-old male, and the hair loss range was S3. If you have atopic dermatitis.
- the results of the scratch test were house dust 3+, tick 3+, camogaya 2+, and ragweed 1+.
- the subject underwent adenoid and tonsillectomy operations at the age of 6 and developed alopecia areata from the age of 7 and showed hair loss on the eyebrows and lower limbs in addition to the head.
- This test subject did not heal even after steroid internal use or topical use.
- the scalp of this test subject's hair loss site was infiltrated with erythema and scales and was accompanied by pruritus.
- this test subject is the same test subject as the test subject of case A5.
- Case B4 The test subject was a 24-year-old woman, the hair loss range was S2, and was a severe patient with multiple alopecia areata. A history of allergic rhinitis. Mother has bronchial asthma. The results of the scratch test were house dust 2+, tick 2+, cedar 2+, camogaya 1+, and ragweed 1+. The alopecia areata from this subject had repeated partial remission and relapse since junior high school. A mild pruritus sensation appeared mainly in the frontal region for six months, and then multiple hair loss spots expanded.
- this test subject even when steroids and carpronium chloride were applied to the hair loss site for 3 months or when an antiallergic agent was taken, hair growth was not observed, and easy hair loss was not improved.
- this test subject is the same test subject as the test subject of case C9.
- Case B13 A test subject is a 39-year-old male and is the same test subject as the test subject of the case of C13 mentioned later.
- the round bald area on the temporal and occipital area of this test subject when 100 ⁇ g / g CNP ointment was applied twice a day, developed hair after one week of application and healed spontaneously after application was stopped after one week. .
- a round hair loss spot was formed at the top of the head.
- the application of the BNP gel was completed in 2 weeks and the progress was observed. However, since no hair growth was observed in the center, 50 ⁇ g / g BNP: 600 ⁇ g / ml betamethasone: 500 ⁇ g from 3 weeks after stopping the BNP gel. When the / ml gentamicin combination was applied once a day for 2 weeks, black bristles grew at a faster hair growth rate.
- Case B5 The test subject is a 50-year-old female, and the hair loss range is S3, which is a severe patient with multiple alopecia areata.
- S3 A history of allergic rhinitis and atopic dermatitis.
- the results of the scratch test were house dust 3+, mite 3+, cedar 3+, camo 2+, and ragweed 2+.
- the alopecia areata of this test subject developed due to stress due to human relations at work from 4 months ago, and began to occur frequently 2 months after the onset.
- This test subject continued to apply steroid steroid lotion and carpronium chloride to the hair loss site for 10 months, but no hair growth was observed, the hair loss was not suppressed, and there was no therapeutic effect.
- the pattern of hair growth was characteristic and began to grow in a double ring shape and recovered to cover the whole in 20 days (see FIGS. 15-1, 15-2 and 16). However, since this subject suffered from the Great East Japan Earthquake on March 11, 2011, treatment with the BNP ointment was discontinued. According to this test subject, it grew to a certain extent, but it stopped growing after the application of BNP ointment was stopped.
- Case B6 The test subject was a 33-year-old female and was a patient with alopecia areata having a hair loss range of S1. The child of this subject suffers from atopic dermatitis. The subject's mother has alopecia areata and a history of allergic rhinitis. The results of the scratch test were house dust 2+, mite 2+, camogaya 2+, and ragweed 2+, which were predisposed to atopy. In this subject, a round hair loss spot appeared 5 months ago, and treatment with topical steroids, application of carpronium chloride, and internal use of antiallergic agents continued for 7 weeks. Therefore, oral steroids were also used, but there was no therapeutic effect. This test subject had a bald area on the left, top and back of the head, and the range of hair loss was S1. In addition, this test subject is the same test subject as the test subject of case C10.
- Case B26 The test subject was a 38-year-old woman and was a patient with alopecia areata having a hair loss range of S1. The child of this subject suffers from atopic dermatitis. In this subject, cousins, nephews and aunt children also suffer from multiple alopecia areata. No scratch test was performed on this subject.
- Case C1 The test subject was a 32-year-old woman with a hair loss range of S3 and a severe patient with multiple alopecia areata. A history of allergic rhinitis. The results of the scratch test were house dust 2+, mite 3+, cedar 2+, camogaya 3+ and ragweed 2+. The alopecia areata of this test subject developed alopecia half a year ago, expanded and occurred frequently, and after 5 months of onset, the entire scalp began to show a tendency to hair loss. In this subject, the change in the workplace triggered the onset of alopecia areata. This subject had no therapeutic effect with the application of carpronium chloride.
- Case C2 The test subject was a 47-year-old female and was a patient with alopecia areata having a hair loss range of S1. This subject has a history of glaucoma. The child of this subject suffers from atopic dermatitis and allergic rhinitis. The results of the scratch test were house dust 3+, mite 3+, cedar 2+, duck 2+, and ragweed 2+. In this test subject, a bald patch appeared on the top of the head one month ago, and thereafter, a bald area was also seen in the frontal and left temporal regions. This is a case where steroid use should be avoided because of a history of glaucoma. The subject suffered from thyroid cancer 7 years ago and has undergone surgery. In addition, this test subject is the same test subject as the test subject of case C11.
- Case C3 The test subject was a 50-year-old woman, and the range of hair loss was S2, which is a severe patient with multiple alopecia areata.
- the subject has a history of atopic dermatitis and allergic rhinitis.
- the subject's mother has a history of alopecia areata and the child has allergic rhinitis and chronic urticaria.
- the results of the scratch test were house dust 1+, tick 1+, camogaya 2+, and ragweed 1+.
- scalp-like scales and erythema with pruritus were observed on the scalp at the hair loss site, and critic alopecia was complicated.
- Case C20 The test subject was a 32-year-old male with androgenetic alopecia. The subject suddenly became 30 years old and the hairline of the M-shaped part of the frontal region suddenly became thin and retreated. A single alopecia areata also developed in the left temporal region 6 weeks before the visit. There are no alopecia patients in this subject's family. This test subject is so-called M-type male pattern alopecia belonging to type III in the Hamilton-Norwood classification. In addition, this test subject is the same test subject as the test subject of case C27.
- Case C4 The test subject was a 50-year-old woman, and the range of hair loss was S2, which is a severe patient with multiple alopecia areata.
- the subject has a history of atopic dermatitis and allergic rhinitis.
- the subject's mother has a history of alopecia areata and the child has allergic rhinitis and chronic urticaria.
- the results of the scratch test were house dust 1+, tick 1+, camogaya 2+ and ragweed 1+.
- scalp-like scales and erythema with pruritus were observed on the scalp at the hair loss site, and critic alopecia was complicated.
- Case C5 The test subject was a 33-year-old woman with a hair loss range of S3 and a severe patient with alopecia areata of B1 with eyebrow hair loss in addition to the head. There is a history of atopic dermatitis, and alopecia due to aggravation of atopic dermatitis is also complicated.
- the results of the scratch test were house dust 2+, mite 1+, camogaya 2+ and ragweed 2+. In this test subject, scalp-like scales and erythema with pruritus were observed on the scalp at the hair loss site, and critic alopecia was complicated.
- Case C6 The test subject was a 22-year-old female, and the hair loss range was S3, which is a severe patient with alopecia areata having a serpentine alopecia type that is said to be intractable.
- the subject has a history of atopic dermatitis and allergic rhinitis.
- the subject's grandfather has atopic dermatitis, and his father, mother, and brother have allergic rhinitis.
- the results of the scratch test were house dust 2+, mite 3+ and camogaya 1+. This test subject developed a hair loss spot more than a year and a half ago, and the hair loss spot was clearly stripped along the outer edge of the hair part without hair growth at all.
- Case C7 The test subject was a 38-year-old woman and was a patient with alopecia areata having a hair loss range of S1. The child of this subject suffers from atopic dermatitis. In this subject, cousins, nephews and aunt children also suffer from multiple alopecia areata. No scratch test was performed on this subject.
- Case C8 The test subject was a 32-year-old female and was a patient with multiple alopecia areata having a hair loss range of S1.
- the results of the scratch test were house dust, mite 1+, cedar 2+, duck 2+ and ragweed 2+.
- Case C9 The test subject was a 24-year-old woman, the hair loss range was S2, and was a severe patient with multiple alopecia areata. A history of allergic rhinitis. Mother has bronchial asthma. The results of the scratch test were house dust 2+, tick 2+, cedar 2+, camogaya 1+, and ragweed 1+. The alopecia areata from this subject had repeated partial remission and relapse since junior high school. A mild pruritus sensation appeared mainly in the frontal region for six months, and then multiple hair loss spots expanded. This test subject showed no hair growth even when steroid or carpronium chloride was applied to the hair loss site for 3 months, or took an antiallergic agent, and the ease of hair removal was not improved. In addition, this test subject is the same test subject as the test subject of case B4.
- Case C10 The test subject was a 33-year-old female and was a patient with alopecia areata having a hair loss range of S1. The child of this subject suffers from atopic dermatitis. The subject's mother has alopecia areata and a history of allergic rhinitis. The results of the scratch test were house dust 2+, tick 2+, camogaya 2+, and ragweed 2+, which were cases with atopic predisposition. In this subject, a round hair loss spot appeared 5 months ago, and treatment with topical steroids, application of carpronium chloride, and internal use of antiallergic agents continued for 7 weeks. Therefore, oral steroids were also used, but there was no therapeutic effect. This test subject had a bald area on the left, top and back of the head, and the range of hair loss was S1. In addition, this test subject is the same test subject as the test subject of case B6.
- the agent was applied twice a day. As a result, hair could not be removed, and remarkable hair growth was observed in any part of the left temporal region, the top of the head and the back of the head 3 weeks after the start of application of the CNP ointment (FIGS. 24-1 and 24-). 2). According to the test subjects, they were annoyed at the speed of hair growth compared to conventional treatments. In this subject, after the application of the CNP ointment was stopped in 21 days, no relapse was observed even after one month.
- Case C11 The test subject was a 47-year-old female and was a patient with alopecia areata having a hair loss range of S1. This subject has a history of glaucoma. The child of this subject suffers from atopic dermatitis and allergic rhinitis. The results of the scratch test were house dust 3+, mite 3+, cedar 2+, camogaya 2+ and ragweed 2+. In this test subject, a bald patch appeared at the top of the head one month ago, and then a bald area was also seen in the frontal and left temporal regions. This is a case where steroid use should be avoided because of a history of glaucoma. The subject suffered from thyroid cancer 7 years ago and has undergone surgery. In addition, this test subject is the same test subject as the test subject of case C2.
- Case C12 The test subject is a 63-year-old female, and the hair loss range is S2, which is a severe patient with multiple alopecia areata. If you have a history of allergic rhinitis and atopic dermatitis. The results of the scratch test were house dust 2+, mite 1+, camogaya 2+, and ragweed 1+. This test subject's alopecia areata lasts more than a year and a half. This test subject continued to apply steroids and carpronium chloride for 10 months to the bald area, but had no effect and no hair growth was observed. In addition, this test subject is the same test subject as the test subject of case B1.
- Case C13 The test subject is a 38-year-old male, and the range of hair loss is S1, and is a patient with multiple alopecia areata. A bald patch appeared in the temporal region from 2 months ago, and a bald area was also seen in the back of the head. There is no history or family history of immune disease. The results of this subject's scratch test were house dust 2+, mite 2+, cedar 2+, duck 2+, and ragweed 1+. The subject took cephalanthin but had no therapeutic effect.
- Case C14 The test subject is a 35-year-old woman, and is a patient with alopecia areata having a hair loss range of S1.
- This test subject has a history of allergic rhinitis, the subject's mother also suffers from allergic rhinitis, and this test subject has a predisposition to atopy.
- the results of this subject's scratch test were house dust 2+, mite 2+, cedar 2+, duck 2+, and ragweed 1+.
- a bald patch appeared on the occipital region three months ago, and then showed a tendency to expand, and the entire occipital region became thin and accompanied by pruritus.
- application of the steroid agent became ugly, and the hair loss range widened.
- Case C15 The test subject was a 52-year-old female and was a patient with severe alopecia areata having a hair loss range of S3. A history of allergic rhinitis. The results of the scratch test were house dust 1+, cedar 2+, camouflage 1+, and ragweed 1+. This test subject continued night shift, and a bald patch appeared on the frontal region about a year ago, and then showed an expanding tendency, and a bald area appeared frequently on the entire scalp. Application of carpronium chloride to the bald patch was continued for 8 months. However, the range of hair loss was widened, but no therapeutic effect was observed. This subject is, erythema on the scalp of the hair loss part, crusts, inflammatory conditions of the scales and the like are the cases that can not be seen. In addition, this test subject is the same test subject as the test subject of case A3.
- Case C36 The test subject was a 57-year-old male, and was a patient with severe alopecia areata having a hair loss range of S2 and a hair loss of eyebrows. This subject has a history of atopic dermatitis.
- the results of the scratch test were house dust 1+, mite 3+, cedar 2+, camogaya 1+, and ragweed 1+.
- This test subject had many hair loss spots about 5 years ago due to work stress.
- the subject continued with liquid nitrogen therapy but had no therapeutic effect at all while the hair loss range expanded. Subsequently, the subject took steroids for internal use and topical use and carpronium chloride for 3 years, but no effect was seen.
- Case C23 The test subject was a 26-year-old female and was a patient with alopecia areata having a single hair loss range of S1.
- the subject has no history of alopecia and the subject's family has no alopecia areata.
- This subject developed a single alopecia areata in the back of the head, visited another clinic, and Linderon TM -V ointment containing 1.2 mg / g betamethasone valerate (Shiono Pharmaceutical Co., Ltd.) Company) was applied for 6 weeks, and it was said that the hair grew slightly, but the size of the bald area increased.
- BNP betamethasone: gentamicin combination on alopecia areata
- Table 7-2 shows the therapeutic effect of BNP: betamethasone: gentamicin combination on alopecia areata.
- Case B14 The test subject was a 31-year-old female and was a patient with alopecia areata having a single hair loss range of S1. This subject has no family with alopecia areata.
- the result of this subject's scratch test was house dust-, mite 1+, cedar 1+, camogaya 1+, and ragweed 2+. He has suffered from multiple alopecia areata 10 years ago. This time, a single alopecia areata developed at the top of the head when he was busy.
- CNP betamethasone: gentamicin combination on alopecia areata
- Table 7-3 shows the therapeutic effect of a CNP: betamethasone: gentamicin combination on alopecia areata.
- Case C21 The test subject was a 51-year-old male and was a patient with alopecia areata having a single hair loss range of S1. This subject has never suffered from alopecia areata and the subject's family has no alopecia areata patients. This subject, alopecia areata group of solitary appeared in the right parietal region from about two months before the visit.
- Delmozol G lotion and calplanin topical solution 5% was completed in 2 months, and after 3 weeks, 50 ⁇ g / g CNP: 600 ⁇ g / ml betamethasone: 500 ⁇ g / ml
- betamethasone 500 ⁇ g / ml
- Application of the CNP: betamethasone: gentamicin combination was completed in 3 weeks, but the hair continued to stretch even after 1 week, and the ground became hidden (FIG. 37).
- Case C22 The test subject was a 33-year-old woman who visited the hospital with a single round bald area on the crown. This subject's hair loss range is a single alopecia areata patient with S1. There are no alopecia areata patients in this subject's family. The results of this subject's scratch test were house dust 2+, mite 1+, cedar 3+, duck 2+, and ragweed 2+. The subject also suffers from alopecia areata when he is in elementary school and junior high school.
- Case A8 The test subject was a 45-year-old man who had thinned hair only at the top of his head from around 44 years old. This test subject is a test subject who has seborrheic alopecia with erythema accompanied by pruritus and seborrheic scales on the scalp of the hair loss site. It belongs to the IIvertex type in the Hamilton-Norwood classification. The subject's father has androgenetic alopecia confined to the crown. Scratch test of this subject, house dust 2+, mite 3+, orchard grass 1+, was ragweed 1+. This test subject is the same test subject as the test subject of case B8.
- Case A9 The test subject was a 75-year-old male, and the top of the head became thin from about 40 to 50 years old.
- This test subject is male pattern alopecia with erythema accompanied by pruritus and seborrheic scales on the scalp at the hair loss site and complicated with seborrheic alopecia. It belongs to type VI in the Hamilton-Norwood classification.
- the subject's father also has androgenetic alopecia.
- house dust 2+, mite 2+, cedar 3+, camogaya 2+, and ragweed 2+ have a history of allergic rhinitis.
- This subject applied minoxidil for 1 year but had no effect.
- This test subject has also been using glycyrrhetinic acid for 2 years but has no effect.
- this test subject is the same test subject as the test subject of case B11.
- a 100 ⁇ g / g ANP gel was applied to the hair loss site at the top of this subject twice a day in the morning and evening for 4 days, but there was no improvement in erythema and seborrheic scales, and an improvement in alopecia was also observed. I could't.
- Case B7 The test subject was a 39-year-old male. At the age of 38, the top of the head was tingling, erythema and scales appeared, the top of the head became thin, and male pattern baldness occurred. It belongs to the IIvertex type in the Hamilton-Norwood classification. The paternal grandfather of this subject has androgenetic alopecia. The results of this subject's scratch test were house dust 3+, tick 3+, cedar 1+, camo 2+, and ragweed 1+.
- Case B8 The test subject was a 45-year-old man who had thinned hair only at the top of his head from around 44 years old. This test subject is male pattern alopecia with erythema accompanied by pruritus and seborrheic scales on the scalp of the hair loss site and complicated with seborrheic alopecia. It belongs to the IIvertex type in the Hamilton-Norwood classification. The subject's father also has androgenetic alopecia confined to the crown. The results of this subject's scratch test were house dust 2+, mite 3+, duck 1+, and ragweed 1+. In addition, this test subject is the same test subject as the test subject of case A8.
- this test subject realized that blood circulation improved, and hair loss decreased from about 5 days, and itching disappeared.
- This test subject increased the hair from about 3 weeks after the start of application of the CNP gel, and increased the hair to an almost normal level after 7 weeks from the start of application.
- this subject is continuing treatment because the hair loss increased and the hair on the top of the head became thin after the application of the CNP gel for 2 to 3 months was stopped.
- Case B9 The test subject was a 42-year-old man who had thinned hair only at the top of his head from about 40 years old. This test subject has mild erythema and scales on the scalp of the hair loss site. It belongs to type V in the Hamilton-Norwood classification. The subject's father and maternal grandfather have androgenetic alopecia. No scratch test was performed on this subject.
- Case B10 The test subject was a 65-year-old male whose hairline on the front and back of the forehead and back of the forehead fell from 30s to 40s. The father also has male pattern baldness. It belongs to type VI in the Hamilton-Norwood classification. As a result of this subject's scratch test, house dust 2+, mite 2+, cedar 1+, camogaya 1+ and ragweed 1+ have a history of atopic dermatitis and allergic conjunctivitis.
- Case B11 The test subject was a 75-year-old male, and the top of the head became thin from about 40 to 50 years old.
- This test subject is male pattern alopecia with erythema accompanied by pruritus and seborrheic scales on the scalp at the hair loss site and complicated with seborrheic alopecia. It belongs to type VI in the Hamilton-Norwood classification.
- the subject's father also has androgenetic alopecia.
- the results of this subject's scratch test were house dust 2+, mite 3+, duck 1+, and ragweed 1+.
- This subject applied minoxidil for 1 year but had no effect.
- the subject says that glycyrrhetinic acid has been in use for two years but has no effect.
- this test subject is the same test subject as the test subject of case A9.
- Case B12 The test subject was a 62-year-old male who had thin hair on the top of the head from around the age of 50 and had scissors-like scales and erythema with pruritus on the scalp at the hair loss site.
- This subject has male pattern baldness with critic alopecia. In the Hamilton-Norwood classification, it belongs to the III vertex type.
- the subject's father and brother also have male pattern baldness.
- the results of this subject's scratch test are house dust 2+, mite 3+, cedar 2+, camogaya 1+, ragweed 2+, and suffers from atopic dermatitis and bronchial asthma.
- My brother has a history of atopic dermatitis and my child has allergic rhinitis.
- Case B15 The test subject was a 44-year-old male who developed M-type alopecia areata from the late 30s. In the Hamilton-Norwood classification, this is a so-called M-type hair loss case belonging to type III. The subject's father also has androgenetic alopecia.
- BNP gel Application of the BNP gel was completed in 2 weeks, and after 5 days, 50 ⁇ g / g BNP: 600 ⁇ g / ml betamethasone: 500 ⁇ g / ml gentamicin combination was applied twice a day for 1 week. As hair loss decreased to 1 or 2, the hair became thicker. Since this subject was busy, even after 3 weeks had passed since the application was stopped, the hair growth state was certainly maintained from before the application.
- Case B16 The test subject was a 46-year-old male who had thinning of the frontal head from the late 30s and thinned the top of the head after 40 years of age. This test subject belongs to type V in the Hamilton-Norwood classification, and the test subject's father and maternal grandfather also have male pattern baldness.
- Case C16 The test subject is a 56-year-old male, and has male pattern baldness, which is thin and soft from the top of the 40s to the frontal region.
- This test subject is a case having both a so-called M-type hair loss site and an O-type hair loss site belonging to the Va type in the Hamilton-Norwood classification.
- the subject who had previously applied 1% minoxidil for years, had no effect, and recently stopped using it because it became red and itchy.
- the scalp at the hair loss site had thinning hair without inflammatory symptoms such as erythema and scales.
- the father and paternal grandfather have androgenetic alopecia.
- the results of this subject's scratch test were house dust, mite 1+, cedar, camogaya, and ragweed.
- Case C17 The test subject was a 59-year-old male with androgenetic alopecia with thinning hair from the top of the head to the frontal region.
- This test subject is a case having both a so-called M-type hair loss site and an O-type hair loss site belonging to type VII in the Hamilton-Norwood classification.
- the scalp at the hair loss site is accompanied by erythema, scales, and scarring, and has a strong itching sensation.
- the subject's father and grandfather also have male pattern baldness.
- the results of this subject's scratch test were house dust 2+, mite 3+, cedar, camogaya 2+, and ragweed 2+.
- the subject had been prescribed steroids and continued topical use for 7 months. However, in only about 1 hour, the pruritus sensation recurred and inflammation did not subside and did not improve.
- Case C24 The test subject was a 48-year-old male with androgenetic alopecia. In this subject, the hairline of the frontal region retreated to M-type and softened from 5 years ago, and the top of the head became thin. In the Hamilton-Norwood classification, it belongs to the III vertex type. This subject has no thin-haired family.
- Case C37 The test subject is a 43-year-old male who has male pattern alopecia in which the anterior temporal region and the top of the head have become thin after becoming 40 years old. This test subject is a case having both a so-called M-type hair loss site and an O-type hair loss site belonging to type V in the Hamilton-Norwood classification.
- Case C38 The test subject was a 33-year-old male, whose hair quality became thin with curly hair in the late 20s and became male pattern baldness after the 30s.
- M-type alopecia belongs to the III vertex type, and the top of the head is thin and the frontal head is depilated.
- the subject's father and maternal grandfather also have male pattern baldness.
- Case C39 The test subject was a 34-year-old male who became thin and became male pattern baldness from the late 20s.
- M-type alopecia which belongs to type V, and the top of the head is thin and the frontal head is depilated.
- the subject's father also has androgenetic alopecia.
- This subject applied a 1% minoxidil solution for 1 year, but had no effect.
- the subject also took biotin and herbal medicine but had no effect.
- 50 ⁇ g / g CNP gel was applied to the frontal region of this test subject twice a day for 3 weeks, hair thickening was confirmed at the top of the head, and the hair became thick and dark.
- the M-shaped part hair growth and hair growth were observed at a slow pace.
- CNP betamethasone: gentamicin combination on androgenetic alopecia
- the therapeutic effect of CNP: betamethasone: gentamicin combination on androgenetic alopecia is shown in Table 10-3 (Case C25).
- Case C25 The test subject was a 75-year-old male with androgenetic alopecia. In this test subject, the hairline of the frontal region retreated to M-type from 5 years ago, and the top of the head began to become thin. In addition, this test subject has been associated with scale hair loss, erythema, and pruritus since half a year ago. This test subject is a case having both a so-called M-type hair loss site and an O-type hair loss site belonging to type VI in the Hamilton-Norwood classification.
- betamethasone 500 ⁇ g / ml gentamicin combination was applied twice a day for 12 days to the frontal and top of this subject, hair loss almost disappeared, and scales and erythema disappeared completely. did.
- CNP clobetasol combination on androgenetic alopecia
- Table 10-4 Therapeutic effect of CNP: clobetasol combination on androgenetic alopecia
- Case C26 The test subject was a 61 year old male with androgenetic alopecia. This test subject is a case with critical hair loss associated with itching and scales, with thinning hair mixed with gray hair on the frontal and top of the head. The subject's father, paternal grandfather, and maternal grandfather also have androgenetic alopecia. The subject suffers from bronchial asthma.
- the test result of this subject's scratch test is a case where the subject has both a so-called M-type hair loss site and an O-type hair loss site belonging to the IVa type in the Hamilton-Norwood classification.
- CNP carpronium chloride combination on male pattern alopecia
- Table 10-5 Therapeutic effect of CNP: carpronium chloride combination on male pattern alopecia
- Case C27 The test subject was a 32-year-old male with androgenetic alopecia. The subject suddenly turned back when he became 30 years old and the M-shaped hairline of the frontal head became thin. A single alopecia areata also developed in the left temporal region 6 weeks before the visit. This subject has no family with alopecia. This test subject is so-called M-type male pattern alopecia belonging to type III in the Hamilton-Norwood classification.
- Case C40 is the same subject as C24, and is a case of androgenetic alopecia. Details of this case are as described as case C24.
- BNP gels and minoxidil multilayer coating of minoxidil multilayer coating male pattern baldness is shown in Table 10-7 (cases B29).
- Case B29 The test subject was a 52-year-old male with male pattern baldness belonging to type IV in the Hamilton-Norwood classification. This test subject has thinned frontal head from around the age of 23, and now the top of the head is also thinned. This subject has no family with alopecia. This subject had no effect with the semi-summer Kobok hot-bath.
- Case C32 is a complication example of male pattern alopecia and seborrheic alopecia, and is the same case as cases A9, B11, and B22.
- Case B17 is the same subject as case A10. Six months after the application of the ANP gel, 50 ⁇ g / g BNP gel was applied to the top of the head 3 to 4 times a day for 3 weeks. The hair increased and hair loss decreased. The hair recovered to such an extent that thin hair was not a concern (FIG. 47).
- Case C18 The test subject was a 27-year-old female and was a patient with postpartum alopecia.
- the patient has a history of atopic dermatitis and is predisposed to atopy.
- the subject's mother suffers from allergic rhinitis, and the subject's mother also has female pattern alopecia with a thin top.
- the results of the scratch test were house dust 3+, mite 3+, cedar 2+, duck 2+, and ragweed 2+.
- This test subject suddenly lost her hair when she gave birth in July. In this test subject, thin hair is conspicuous from the top of the head to the front of the head.
- the subject continued to apply steroids and carpronium chloride for 5 months, but the hair loss remained high and the thinning hair at the top of the head was not improved.
- Case B18 The test subject is a 56 year old female and is a patient with female pattern alopecia. This test subject had a lot of cut hair and hair loss, and diffuse hair loss centered on the midline was observed. The subject's father, grandfather, and brother have male pattern baldness.
- a BNP gel with a concentration of 50 ⁇ g / g was applied to the top of the subject's head. From about two weeks after the start of application, hair growth and hair growth were remarkably observed, and the number of hair loss attached to the hand during shampooing decreased to about 10 during application. This test subject eventually increased the hair so that the skin could not be seen. After that, even if it has not been used for 4 months, it can be kept in a state where it is still hard and has little hair loss.
- Case B19 The test subject is a 59-year-old female and is a patient with female pattern alopecia. This test subject was in his 50s, and the thinning hairs at the frontal part became conspicuous.
- Case B20 The test subject is a 50-year-old female and is a patient with female pattern alopecia. This test subject had thinned from several years ago from the top of the head to the frontal region, and the division has expanded. The mother of this subject also has female pattern alopecia, and the father has male pattern alopecia.
- “Dermosol-G Lotion” (Iwaki Pharmaceutical Co., Ltd.) containing 1200 ⁇ g / ml betamethasone valerate and 1000 ⁇ g / ml gentamicin sulfate was continuously applied to the top of this subject for 8 weeks. However, the thinning hair was not improved at all.
- the application of the CNP gel was discontinued in 2 weeks, and after 2 weeks, 50 ⁇ g / g CNP: 600 ⁇ g / ml betamethasone: 500 ⁇ g / ml gentamicin combination was applied twice a day for 2 weeks. The state was maintained. After the application of the 50 ⁇ g / g CNP: 600 ⁇ g / ml betamethasone: 500 ⁇ g / ml gentamicin combination was discontinued in 2 weeks, even after 2 weeks, the thin hair was not noticeable and kept normal.
- Case B27 The test subject was a 66-year-old woman who became thin from 65 years old. This is a female pattern alopecia combined with seborrheic alopecia with prominent seborrheic scales on the scalp. This test subject has thin hair from the top of the head to the frontal head and the left M-shaped part, and the background is quite transparent. This test subject had a great deal of hair loss, and was easily removed just by touching. The subject's father and brother have male pattern baldness.
- Case C19 The test subject is a 56 year old female and is a patient with female pattern alopecia.
- the subject's father is male pattern alopecia
- the subject's mother is female pattern alopecia.
- the results of the scratch test were house dust 2+, tick 2+, cedar 1+, duck 1+, and ragweed 1+. This subject has been thinned at the top of the head for 10 years. This subject had no effect with topical use of steroids and carpronium chloride.
- Case C28 The test subject is a 62-year-old female and is a patient with female pattern alopecia.
- the scalp began to become bulky around April after the Great East Japan Earthquake on March 11, 2011, and became thin from the frontal region to the top of the head.
- the father of this test subject has been in a total head loss state due to androgenetic alopecia since about 35 years old.
- Case C29 The test subject is a 60-year-old female and is a patient with female pattern alopecia. In this test subject, scales and pruritus appeared one year ago, and the hairline of the frontal head became thin.
- Case A11 is a complication example of male pattern alopecia and seborrheic alopecia, and is the same case as cases A8 and B8. The details of this case are as described in cases A8 and B8.
- 100 ⁇ g / g ANP gel was applied to the entire hair loss site at the top of the head twice in the morning and evening, the second day Strong itching, hair loss increased, hair loss range expanded, seborrheic exacerbation of the scalp and erythema appeared, and no hair growth was observed.
- Case A12 is a complication example of male pattern alopecia and seborrheic alopecia, and is the same case as cases A9 and B11. The details of this case are as described in cases A9 and B11, and 100 ⁇ g / g ANP gel was applied to the hair loss site at the top of the head twice in the morning and evening for 4 days. There was no improvement in seborrheic scales and no improvement in alopecia.
- Case B21 is a complication example of male pattern alopecia and seborrheic alopecia, and is the same case as cases A8 and B8. The details of this case are as described for cases A8 and B8.
- Case B22 is a complication example of male pattern alopecia and seborrheic alopecia, and is the same case as cases A9 and B11. The details of this case are as described for cases A9 and B11.
- Case A13 is a complication example of alopecia areata and critical alopecia and is the same case as cases A6, C3, C4, and C30. However, the CNP ointment was applied to the crown. The details of this case are as described in cases A6, C3, and C4, and even if 100 ⁇ g / g ANP gel was applied for 2 weeks, there was no effect, and bulky scales increased and pruritus occurred. Yes, the hair loss range has rather expanded.
- Case B23 The test subject was an 81-year-old man who had thinned hair from the frontal region to the top of the head for 3 years. This is a complication of senile alopecia and critical alopecia with scaly scales on the scalp.
- a 50 ⁇ g / g BNP gel was applied to the frontal region and the top of the subject for 2 weeks, followed by a 1-week withdrawal period, and 200 ⁇ g / g BNP gel was applied once a day for 5 days.
- the crippling desquamation was relieved, the soft hairs became dark and blackened, and the thin hairs were greatly improved (FIG. 51).
- Case B28 The test subject was a 59-year-old male with critical alopecia. This test subject is in a thin state with almost no hair from the frontal region to the top of the head. Two years ago, she became thin and applied Reup X5 (trademark) containing 0.05 g / ml minoxidil twice a day for a year and a half. Hair loss and thinning of the hair suddenly worsened from the front. This test subject was in a state in which a large amount of hair adhered to and removed from the scalp scales during hair washing.
- Case C30 is a complication example of alopecia areata and critical alopecia and is the same case as cases A6, C3, C4, and A13. However, the CNP ointment was applied to the right frontal region. The details of this case are as described in cases A6, C3, and C4. The application recovered smoothly even after the application was stopped twice a day for 3 weeks by applying 100 ⁇ g / g CNP gel. No relapse was observed at the site of application even after 8 months.
- Case C31 The test subject was a 42 year old male and was a patient with critical alopecia. From the late 30s, the forehead and the crown became thin.
- “Nitrazen Cream 2%” (Iwaki Pharmaceutical Co., Ltd.) containing 2% of ketoconazole, an antifungal agent, and Betamethasone Yoshi, a 1.2 mg / g synthetic adrenocortical hormone “Betnoval G Ointment Cream” (Sato Pharmaceutical Co., Ltd.) containing herbic acid ester and 1 mg / g antibiotic gentamicin has been applied, but it was not effective at all.
- the dandruff was thickly attached from the front, and the thinning hair was further deteriorated.
- Case C33 is a complication example of alopecia areata and critical alopecia and is the same case as cases A6, C3, C4, A13, and C30. However, the CNP ointment was applied to the right frontal region. The details of this case are as described for cases A6, C3, and C4. By applying 100 ⁇ g / g CNP ointment twice a day for 2 weeks, clear hair growth was observed, The scalp erythema and scales also disappeared.
- test subject is a 74-year-old male with senile alopecia with dandruff, lots of hair loss, thin hair on the entire head, and conspicuous gray hair.
- the subject also has a strong itch on the scalp, a lot of dandruff, and a lot of hair loss.
- the ANP gel was discontinued in one week, and 50 ⁇ g / g CNP gel was applied twice a day from the next day, and erythema, scales and pruritus were alleviated by application for 2 days. Subsequently, when 50 ⁇ g / g CNP gel was continuously applied twice a day for a period of 4 weeks, obvious hair thickening was observed especially in the frontal region, and hair loss disappeared (FIG. 54). Moreover, the hair which grew was black hard hair, and even if it rubbed strongly, it did not come off. It was surprising that the effect of hair thickening was seen with CNP gel even at the age of 74 years.
- Case B24 is a complication example of senile alopecia and critical alopecia and is the same case as case B23. Therefore, this case is as described in detail as case B23.
- Case C34 The test subject was a 70-year-old woman, and the head of the head became thin from 68 years old. According to the test subject, the skin at the top of the head with thinning hair is shrunken and painless enough to touch. Therefore, when a CNP gel with a concentration of 50 ⁇ g / g was applied twice a day for 3 days, the pain on the scalp was alleviated and hair loss was reduced. Thereafter, when the application was continued for another 3 days, the erythema of the scalp disappeared, and pruritus and pain were not recognized, and increased hair was observed.
- Case B25 The test subject is a 54 year old female. The subject was diagnosed with malignant lymphoma and received 6 courses of R-CHOP therapy during the period from April to September 2011.
- the R-CHOP therapy is a kind of cocktail therapy using a plurality of chemotherapeutic agents.
- R-CHOP therapy is a drip infusion of rituximab which is a mouse-human chimeric monoclonal antibody against CD20 which is a human B cell surface antigen.
- prednisolone tablets On the second day, on the second day, oral administration of prednisolone tablets, a synthetic corticosteroid, intravenous administration of vincristine, a microtubule polymerization inhibitor, and doxorubicin, a DNA and RNA synthesis inhibitor
- days 3-6 Following intravenous injection and intravenous injection of cyclophosphamide, a prodrug of DNA synthesis inhibitor, on days 3-6, only prednisolone tablets were taken after each meal, and days 7-21 Is a treatment that repeats this dosing cycle, with the dosing schedule for the drug holiday as one course.
- the subjects started to lose their hair from the second week of the first course, and passed through in July when the fourth course ended. Although the hair began to grow gradually after the treatment was completed in September, it was pure white hair and the hairline on the left side receded and became very thin.
- a BNP gel with a concentration of 100 ⁇ g / g was applied to the left hairline part twice a day for one week. After two weeks, black bristles grew in the thinned state like white hair, and gradually to Mashike, it began to black hair to the hairline part that had retreated to the M-type looks aligned grows round. In the BNP gel application site of the left hairline M type site, all hairs that grew were black hairs. After 3 months, no hair loss reappeared and no whitening occurred.
- Case C35 The test subject was a 47 year old female. After undergoing surgery for endometrial cancer in November 2009, the subjects received 6 courses of treatment with cisplatin, a cancer chemotherapeutic agent, and completed cancer chemotherapy in March 2010. The subject suffered from total head hair loss following treatment with cisplatin, and after about 1 year had passed since the end of treatment with cisplatin, thin, soft, short hair has grown from around May 2011. From the front to the top of the head, It recovered only to the state of thinning hair. In contrast, the subject applied carpronium chloride for 6 months, but no effect was seen.
- the therapeutic agent for alopecia of the present invention has a remarkable therapeutic effect when CNP or BNP is used as an active ingredient, and hair growth is almost certainly achieved by application twice a day for one week, and application for two weeks.
- the hair became bristle and became difficult to see after 4 weeks of application.
- it is not necessary to continue painting after the soft hair has grown, and the soft hair became thicker and thicker and became hardened and continued to grow.
- the therapeutic agent for alopecia of the present invention containing CNP as an active ingredient can more reliably suppress inflammation at the hair loss site than when BNP is used as the active ingredient, and the amount of hair loss can be reduced from 1 to several days. Dramatically decreased and hair growth occurred earlier.
- the therapeutic agent for alopecia of the present invention containing BNP as an active ingredient is characterized in that black hard hair often grows.
- the therapeutic agent for alopecia of the present invention was effective only for alopecia in which erythema, scales, seborrheic desquamation, etc. were not observed on the scalp when ANP was used as an active ingredient. There were many cases where teams and itching were worse and worse than before application.
- the therapeutic agent for alopecia of the present invention is effective for alopecia areata and male pattern alopecia and can cause hair growth while suppressing inflammation of seborrheic alopecia and erosion alopecia.
- Drastically reduced dandruff and reduced itching It was also confirmed that hair regeneration was promoted in female pattern alopecia, postpartum alopecia, and senile alopecia, and that black hair growth was promoted in cancer chemotherapy-induced alopecia.
- the therapeutic agent for alopecia of the present invention has a long duration of improvement effect even in male pattern alopecia, female pattern alopecia, seborrheic alopecia, critical alopecia and senile alopecia, and at least after the end of application The hair loss did not reignite at the application site for over 2 months.
- alopecia areata and cancer chemotherapeutic agent alopecia
- topical alopecia treatment of the present invention for 1 to 3 weeks, the hair growth state continues to improve even after discontinuation of use, and healed. Alopecia did not reignite at the application site.
- the therapeutic agent for alopecia of the present invention is alopecia areata, androgenetic alopecia, seborrheic alopecia, fertility alopecia, female pattern alopecia, postpartum alopecia, senile alopecia and cancer chemotherapeutic agents Since it was confirmed that it had a remarkable effect in the treatment of alopecia, it was proved that it is effective not only for treating these but also for treating almost all alopecia.
- each alopecia has a completely different onset mechanism, and it is clear that it is useful for the treatment of alopecia in general because it is effective for various different alopecias.
- the subject whose effectiveness of the therapeutic agent for alopecia of the present invention has been confirmed does not include the subject himself or the subject having a history or complication of immune disease in the relative of the subject.
- the therapeutic agent for alopecia of the present invention can be applied to a subject with a genetic background, history or complications of an immune disease, as well as to a subject who does not have it. Useful.
- the effectiveness of the therapeutic agent for alopecia of the present invention also shows some rules between the result of the scratch test of the subject whose effectiveness was confirmed.
- the therapeutic agent for alopecia of the present invention is equally effective regardless of whether the subject has any allergic predisposition or an allergic predisposition in the first place.
- Therapeutic agent for alopecia of the present invention was confirmed to have a significant effect in the treatment of alopecia areata and male pattern baldness.
- QOL quality of life
- the therapeutic agent for alopecia of the present invention is a single type or severe multiple alopecia areata of S2 or more, a case in which hair loss is combined other than the head, a complication example of atopic disease that is said to be intractable, serpentine hair loss It was also found to be very effective for the disease.
- the therapeutic agent for alopecia of the present invention can restore the hair of a postpartum alopecia patient who does not heal spontaneously to the same state as before delivery even after the second half year of delivery, and is treated with steroids or carpronium chloride It was also proved to be effective for resistant subjects.
- the therapeutic agent for alopecia of the present invention is also effective for female pattern alopecia, and can recover hair to the extent that it does not seem to be anxious after application for 1 to 2 weeks.
- Carpronium chloride, steroid, antifungal It has also been shown to be effective in patients who are resistant to treatment.
- the therapeutic agent for alopecia of the present invention may return to thin hair after about one month from application stop, but by applying again, the hair recovers as in the previous application, It was confirmed that there were no side effects.
- the therapeutic agent for alopecia of the present invention was found to significantly improve erythema, seborrheic scales and pruritus at the hair loss site of seborrheic alopecia and reduce hair loss.
- the therapeutic agent for alopecia of the present invention can eliminate erythema and scales of critical alopecia, can cause black bristles, and does not reignite even after 1 month from application discontinuation. It was done.
- the therapeutic agent for alopecia of the present invention was also effective for critical alopecia resistant to antifungal agents and steroids.
- the therapeutic agent for alopecia of the present invention has been shown to relieve pain and itching of the scalp, relieve erythema and critical desquamation, and grow black hair even for senile alopecia.
- the therapeutic agent for alopecia of the present invention is also effective for cancer chemotherapeutic alopecia, and can cause black hair to grow even in parts that have become gray hair, and more than 2 months after discontinuation of application It was confirmed that the hair growth state was maintained even after elapse.
- the effect of the therapeutic agent for alopecia of the present invention exhibited a remarkable therapeutic effect on alopecia using any of BNP and CNP as an active ingredient.
- the hair growth effect was exhibited even with ANP as an active ingredient only when erythema, scales, seborrheic erythema, seborrheic desquamation, and sputum desquamation were not seen on the scalp.
- two or more NP chimeric peptides selected from ANP, BNP, and CNP also show the same therapeutic effect on alopecia.
- ANP and BNP activate the NPR-A receptor to cause vasodilatory action, diuretic action and cell growth inhibitory action, and CNP acts to inhibit vascular smooth muscle cell proliferation via the NPR-B receptor.
- the therapeutic agent for alopecia of the present invention comprising CNP or BNP as an active ingredient exerted a particularly remarkable alopecia therapeutic effect, and a chimera of BNP and CNP. It is sufficient to understand that the peptide exhibits a similar alopecia treatment effect.
- Alopecia areata develops in young women at the same frequency as men, and despite the fact that their appearance is greatly impaired, long-term expectation of local steroid injection and intentional skin irritation There was only a violent treatment method.
- the alopecia treatment agent of the present invention is particularly effective for alopecia areata, has no side effects in BNP and CNP, and the effect is not seen only during the application period but remains in an improved state after application is discontinued
- a bald area is born in a site that has not been applied, relapse of the applied site has not occurred in experienced cases, which is a great hope for patients suffering from alopecia areata.
- the therapeutic agent for alopecia of the present invention containing natriuretic peptide (NP) as an active ingredient is alopecia areata, male pattern alopecia, female pattern alopecia, postpartum alopecia, seborrheic alopecia, To promote hair growth, hair growth, and hair growth in hair loss sites of epileptic alopecia patients, senile alopecia patients, cancer chemotherapeutic alopecia patients, and alopecia patients due to radiation exposure to improve alopecia markedly It has no side effects such as pruritus, irritation, feminization, etc., and even if it is stopped, the alopecia treatment effect is not lost for a long time.
- the therapeutic agent for alopecia of the present invention is extremely useful for alopecia in which sufficient treatment effect cannot be obtained by conventional minoxidil or finasteride, and alopecia that develops due to excessive immune reaction or immune abnormality. Its usefulness can be expected as an effective therapeutic agent.
- the therapeutic agent for alopecia of the present invention can drastically improve severe alopecia of the head of an adult who suffers from treatment and interferes with social life without any side effects.
- the therapeutic agent for alopecia of the present invention is not only effective for refractory alopecia, but the same effect is observed not only in adults but also in teenagers regardless of gender.
- the therapeutic agent for alopecia of the present invention can be expected to be put to practical use as a new androgenetic alopecia therapeutic agent that replaces minoxidil and finasteride, and further, as a therapeutic agent for alopecia areata that has not been effective for a long time.
- the practical application can be expected greatly.
Abstract
Description
なお、以下、治療剤および/または予防剤を単に治療剤と記す。
脱毛症は、体毛が減少する病気である。脱毛症における体毛の減少は、頭髪だけではなく全身のあらゆる場所で生じうる。その多くは生死に関わるものではないが、その外見上の問題により深刻な精神的苦痛を伴うことから、脱毛症の優れた予防剤および治療剤が望まれている。また、脱毛症は髪の色の退色を伴うことが多いので、脱毛症に伴う髪の色の退色の予防剤および治療剤が望まれている。さらに、脱毛症は、髪が細くなったり髪が短くなるなどの髪質の劣化を伴うことが多いので、脱毛症に伴う髪質劣化の予防剤および治療剤が望まれている。
男性型脱毛症は、年齢とともに発生頻度が高くなり、日本人の場合、20代で約10%、30代で20%、40代で30%、50代以降で40数%が発症する(非特許文献1)。前頭部や頭頂部などの男性ホルモン感受性毛包においては、他の場所の体毛とは逆に、男性ホルモンによって軟毛化現象を引き起こすことによって頭髪が薄くなる。生理的な現象ではあるが、外見上の印象を大きく左右するので社会的な影響は大きい。最近になり男性型脱毛症に有効なミノキシジル外用薬およびフィナステリド内服薬が開発され、皮膚科診療においても積極的に使用されるようになってきたが、依然として十分な治療効果が得られているとは言いがたい。
円形脱毛症は後天性脱毛症の中で最も頻度が高い疾患で、アメリカでは人口の0.1~0.2%に発生しており、本邦でも同程度と思われる。円形脱毛症はどんな年齢でも罹患する。円形脱毛症患者の4分の1は15歳以下で発症し、比較的に小児に多い脱毛症である。全頭型や全身型などの重度の円形脱毛症も小児に比較的に多くみられる。円形脱毛症に男女差はない。円形脱毛症患者の約4分の1の患者の爪には特徴的な症状として、小さな凹み、横の溝などの変化がみられる。円形脱毛症は、基本的に脱毛面積が広いほど難治性であることから、脱毛面積に基づいた重症度分類も考えられてきた(非特許文献4)。円形脱毛症患者は脱毛の他に身体的障害はないことが多いが、患者の悩みは深く、精神的ダメージやQOLの低下は大きい。そのため、あらゆる方法を用いて治療しなくてはならない皮膚疾患として位置づけられるが、有効な治療方法はほとんどないのが現状である。
[1]. 通常型円形脱毛症
単発型:脱毛班が単発のもの
多発型:複数の脱毛班を認めるもの
[2]. 全頭脱毛症:脱毛巣が全頭部に拡大したもの
[3]. 汎発性脱毛症:脱毛が全身に拡大するもの
[4]. 蛇行状脱毛症:頭髪の生え際が帯状に脱毛するもの
に分類される。
S0: 脱毛がみられない。
S1: 脱毛巣が頭部全体の25%未満
S2: 脱毛巣が25~49%
S3: 脱毛巣が50~74%
S4: 脱毛巣が75~99%
S5: 100%脱毛
B0: 頭部以外の脱毛なし
B1: 頭部以外に部分的な脱毛がみられる
B2: 全身すべての脱毛
と規定されており、円形脱毛症は脱毛巣の範囲が広いほど重症で難治である。
女性型脱毛症では、ホルモンバランスが崩れたことにより髪の成長期が短くなり、休止期が長くなってしまう。そのため、1つの毛穴から出る髪の本数が減ったり、髪そのものが健常状態の半分以下の細さになったり、髪の色が薄くなったりする。結果として、頭頂部を中心に髪の隙間から頭皮が見えてしまう状態、つまり全体的に薄くなるパターンとして観察される。
多くの女性は、妊娠中には毛髪が太くなり、出産後に授乳する際には脱毛が起きることを経験する。分娩後脱毛症の原因は明確であるので、診断も容易であり、多くの場合は自然治癒するので、特に治療は行なわれない。しかし、出産経験者の約4割が分娩後脱毛症を経験しているとされており、無視できない数の患者が存在する。また、分娩後脱毛症の脱毛の程度、および、その回復度合いには個人差があり、産後のストレスなどが重なると、まれに抜け毛が止まらない場合がある。この場合、ステロイドを長期間使用してしまうと発毛が困難になるケースが多く、注意を要する。
脂漏性脱毛症においては、毛穴から皮脂が絶えず大量に分泌されて、肉眼でも判るほどに毛穴を塞いでしまっている。そのため、皮脂を除去すると毛穴が炎症で赤くなっており、この炎症によって脱毛するので、診断は比較的容易である。
粃糠性脱毛症は、フケがカサブタ状になり、毛穴を塞いで炎症を起こしてしまうほど大量のフケが異常発生してしまう疾病であるので、その診断は比較的容易である。その原因としては、ホルモンバランスの異常によって頭皮の常在菌が異常繁殖し、それが元となって脱毛に繋がるものであると言われている。
老人性脱毛症は男女の差に関わり無く、加齢に伴って頭部全体を含む全身の体毛に抜け毛・薄毛が生じる脱毛症である。老人性脱毛症の症状としては、頭皮が乾燥し、皮膚から血管が透けて見えるという特徴が見受けられることが多い。老人性脱毛症の原因は、老化によって身体が新しい細胞を作る力が衰えていく事が原因であるために治療は難しい。現在ある老人性脱毛症の治療としては、せいぜい、頭皮のマッサージなどで毛乳頭を活性化させることで発毛の可能性を向上させることていどであり、治療法は無きに等しい。
癌化学療法剤性脱毛症は、癌化学療法剤が細胞分裂を障害することにより、細胞分裂が活発であるがん細胞を選択的に殺すと同時に、同様に細胞分裂が活発である毛母細胞をも障害することによって生じる脱毛症である。
ナトリウム利尿ペプチド(NP;natriuretic peptide)としては、3種類のナトリウム利尿ペプチドファミリーが知られており、具体的には、心房性ナトリウム利尿ペプチド(ANP;atrial natriuretic peptide)、B型ナトリウム利尿ペプチド(BNP;B-type natriuretic peptide)、C型ナトリウム利尿ペプチド(CNP;C-type natriuretic peptide)であり、それぞれ順に、28残基、32残基、22残基のアミノ酸からなる物が主として知られている。
ANPは主として心房で合成され、BNPは主として心室で合成され、心臓から全身へ分泌される。血中を循環しているANP、BNPは、ほぼ100%心臓由来であるといわれている。これらANP、BNPは、高血圧、心肥大、心不全、心筋梗塞、弁膜症、不整脈、肺高血圧などの病態に深く関与しているとの報告がなされている。
CNPは最初に脳内より発見されたことから、脳神経ペプチドとして機能していると考えられていたが、その後末梢にも存在することが明らかになった。特に、血管壁においては、平滑筋細胞にCNP特異的受容体が多いこと、単球/マクロファージ系細胞および内皮細胞がCNPを産生すること、などから、CNPは血管壁の局所因子として平滑筋細胞の増殖抑制に関与するものと考えられている。このことから、虚血性心疾患の患者が経皮的冠動脈形成術(PTCA)を受けた後に一定の頻度で発生し臨床的に問題となっている血管内再狭窄を、CNPの投与によって予防できる可能性について、現在臨床応用が検討されている。
NPの受容体としては、グアニレートシクラーゼドメインを有するNPR-A受容体(別名、GC-A)、グアニレートシクラーゼドメインを有するNPR-B受容体(別名、GC-B)、グアニレートシクラーゼドメインを有さないNPR-C受容体の3種類の受容体が知られており、ANPはNPR-A受容体およびNPR-C受容体に、BNPはNPR-A受容体およびNPR-C受容体に、CNPはNPR-B受容体およびNPR-C受容体に、それぞれ結合しうることが知られている。
ナトリウム利尿ペプチドは、歴史的には、まず、心房が分泌するペプチドとしてANPが発見されるとともにその血管拡張作用および利尿作用が注目を集めた。その後、ANPに類似するペプチドとしてBNPおよびCNPが見出された。このような歴史的経緯から、ナトリウム利尿ペプチドと免疫との関連については、心血管系に関連したものに関心が注がれてきた。
[1] ナトリウム利尿ペプチド(NP)を有効成分として含有する脱毛症、フケ、掻痒、白髪および脂漏性頭皮の治療剤または予防剤、発毛剤、育毛剤、抜け毛進行予防剤、薄毛進行予防剤、毛成長促進剤、発毛促進剤、養毛剤、産後または病後の脱毛治療剤または予防剤。
[2] 脱毛症が、円形脱毛症、男性型脱毛症、分娩後脱毛症、女性型脱毛症、脂漏性脱毛症、批糠性脱毛症、抜毛症、癌化学療法剤性脱毛症、老人性脱毛症、または、薬物に起因する脱毛症である、[1]に記載の治療剤または予防剤。
[4] ナトリウム利尿ペプチド(NP)が、C型ナトリウム利尿ペプチド(CNP)、B型ナトリウム利尿ペプチド(BNP)またはA型ナトリウム利尿ペプチド(ANP)のいずれかである、[1]の治療剤または予防剤。
[6] ナトリウム利尿ペプチド(NP)がCNP-22である、[1]に記載の治療剤または予防剤。
[8] ナトリウム利尿ペプチド(NP)がBNP-32である、[1]に記載の治療剤または予防剤。
前記CNPが、CNP-22、CNP-53、1~5個の任意のアミノ酸が欠失、置換若しくは付加したCNP-22のアミノ酸配列中の5アミノ酸以上の連続する任意のアミノ酸配列を含むペプチド、または、1~5個の任意のアミノ酸が欠失、置換若しくは付加したCNP-53のアミノ酸配列中の5アミノ酸以上の連続する任意のアミノ酸配列を含むペプチドからなる群より選択されるペプチドであり、
前記BNPが、BNP-26、BNP-32、BNP-45、または、1~5個の任意のアミノ酸が欠失、置換若しくは付加したBNP-26のアミノ酸配列中の5アミノ酸以上の連続する任意のアミノ酸配列を含むペプチド、1~5個の任意のアミノ酸が欠失、置換若しくは付加したBNP-32のアミノ酸配列中の5アミノ酸以上の連続する任意のアミノ酸配列を含むペプチド、1~5個の任意のアミノ酸が欠失、置換若しくは付加したBNP-45のアミノ酸配列中の5アミノ酸以上の連続する任意のアミノ酸配列を含むペプチドからなる群より選択されるペプチドであり、
前記ANPが、ANPまたは1~5個の任意のアミノ酸が欠失、置換若しくは付加したANPの、アミノ酸配列中の5アミノ酸以上の連続する任意のアミノ酸配列を含むペプチドであり、
かつ、CNP活性、BNP活性またはANP活性を有するキメラペプチド、あるいは、前記のNPのキメラペプチドの誘導体である、[1]に記載の治療剤または予防剤。
[15] フィナステリドをさらに含む、[1]に記載の治療剤または予防剤。
[16] エストロゲン、エストラジオールまたはプロゲステロンからなる群から選択される少なく一つの女性ホルモン剤をさらに含む、[1]に記載の治療剤または予防剤。
[19] 脱毛症に伴って本来の髪の色よりも薄い色調の髪に変化した発毛状態を本来の髪の色による発毛に回復させる、[1]に記載の治療剤または予防剤。
[21] 髪質を硬毛化させる、[1]に記載の治療剤または予防剤。
[22] フケの発生または頭皮の脂漏性を抑制する、[1]に記載の治療剤または予防剤。
[24] 男性型脱毛症が、脂漏性脱毛症または批糠性脱毛症を合併した男性型脱毛症である、[2]に記載の治療剤または予防剤。
[26] 脱毛部位が前頭部または頭頂部である、[1]または[23]に記載の治療剤または予防剤。
[28] 円形脱毛症が、通常型円形脱毛症、全頭脱毛症、汎発性脱毛症または蛇行状脱毛症である、[1]に記載の治療剤または予防剤。
[30] 自己免疫疾患が、慢性円板状エリテマトーデス、限局性強皮症、天疱瘡、類天疱瘡、妊娠性疱疹、線状IgA水疱性皮膚症、後天性表皮水疱症、尋常性白斑、サットン後天性遠心性白斑のいずれかである、[29]に記載の治療剤または予防剤。
[32] 脱毛症が、アトピー性疾患の既往または合併を有する対象の脱毛症である、[1]に記載の治療剤または予防剤。
[34] 脱毛症が、紅斑、鱗屑または痂皮を伴う脱毛症である、[1]に記載の治療剤または予防剤。
[36] 脱毛症が、フィラグリン遺伝子異常を有し、アトピー性皮膚炎の既往または合併を有する対象の脱毛症である、[1]に記載の治療剤または予防剤。
[41] 脱毛症が、ステロイド離脱困難状態に至った対象の脱毛症である、[1]に記載の治療剤または予防剤。
[43] 脱毛症が、塩化カルプロニウムに治療抵抗性を示す脱毛症である、[1]に記載の治療剤または予防剤。
[45] 脱毛症が、5α-リダクターゼ2型阻害剤を使用できない対象における脱毛症である、[1]に記載の治療剤または予防剤。
[47] 脱毛症が、抗ヒスタミン薬に治療抵抗性を示す脱毛症である、[1]に記載の治療剤または予防剤。
[49] 脱毛症が、ミノキシジルに治療抵抗性を示す脱毛症である、[1]に記載の治療剤または予防剤。
[51] 5α-リダクターゼ2型阻害剤が、フィナステリドである、[50]に記載の治療剤または予防剤。
[53] 円形脱毛症が、S1またはB0以上の脱毛症である、[2]に記載の治療剤または予防剤。
[54] 円形脱毛症が、S2以上の脱毛症である、[2]に記載の治療剤または予防剤。
[56] 円形脱毛症が、S4以上の脱毛症である、[2]に記載の治療剤または予防剤。
[58] 円形脱毛症が、B0の脱毛症である、[2]に記載の治療剤または予防剤。
[60] 円形脱毛症が、B2の脱毛症である、[2]に記載の治療剤または予防剤。
[62] 2週間以上の塗布で治療効果が得られる、[1]に記載の治療剤または予防剤。
[64] 塗布を中止しても1ヶ月以上の期間にわたって再燃しない、[1]に記載の治療剤または予防剤。
[66] 塗布を中止しても6ヶ月以上の期間にわたって再燃しない、[1]に記載の治療剤または予防剤。
[69] ナトリウム利尿ペプチド(NP)の含有量が、1~1000μg/gである、[1]に記載の治療剤または予防剤。
[71] ナトリウム利尿ペプチド(NP)の含有量が、20~300μg/gである、[1]に記載の治療剤または予防剤。
[73] ナトリウム利尿ペプチド(NP)の含有量が、50~100μg/gである、[1]に記載の治療剤または予防剤。
ナトリウム利尿ペプチド(NP)が、分子内ジスルフィド結合によって環状構造を形成する、ANP、BNPまたはCNPから選択される2以上のナトリウム利尿ペプチド(NP)のキメラペプチドであって、
前記CNPが、CNP-22、CNP-53、1~5個の任意のアミノ酸が欠失、置換若しくは付加したCNP-22のアミノ酸配列中の5アミノ酸以上の連続する任意のアミノ酸配列を含むペプチド、または、1~5個の任意のアミノ酸が欠失、置換若しくは付加したCNP-53のアミノ酸配列中の5アミノ酸以上の連続する任意のアミノ酸配列を含むペプチドからなる群より選択されるペプチドであり、
前記BNPが、BNP-26、BNP-32、BNP-45、または、1~5個の任意のアミノ酸が欠失、置換若しくは付加したBNP-26のアミノ酸配列中の5アミノ酸以上の連続する任意のアミノ酸配列を含むペプチド、1~5個の任意のアミノ酸が欠失、置換若しくは付加したBNP-32のアミノ酸配列中の5アミノ酸以上の連続する任意のアミノ酸配列を含むペプチド、1~5個の任意のアミノ酸が欠失、置換若しくは付加したBNP-45のアミノ酸配列中の5アミノ酸以上の連続する任意のアミノ酸配列を含むペプチドからなる群より選択されるペプチドであり、
前記ANPが、ANP-28または1~5個の任意のアミノ酸が欠失、置換若しくは付加したANPの、アミノ酸配列中の5アミノ酸以上の連続する任意のアミノ酸配列を含むペプチドであり、
かつ、CNP活性、BNP活性またはANP活性を有するキメラペプチド、あるいは、その誘導体をも意味する。
ナトリウム利尿ペプチド(NP)が、分子内ジスルフィド結合によって環状構造を形成する、CNPとBNPのキメラペプチドであって、
前記CNPが、CNP-22、CNP-53、1~5個の任意のアミノ酸が欠失、置換若しくは付加したCNP-22のアミノ酸配列中の5アミノ酸以上の連続する任意のアミノ酸配列を含むペプチド、または、1~5個の任意のアミノ酸が欠失、置換若しくは付加したCNP-53のアミノ酸配列中の5アミノ酸以上の連続する任意のアミノ酸配列を含むペプチドからなる群より選択されるペプチドであり、
前記BNPが、BNP-26、BNP-32、BNP-45、または、1~5個の任意のアミノ酸が欠失、置換若しくは付加したBNP-26のアミノ酸配列中の5アミノ酸以上の連続する任意のアミノ酸配列を含むペプチド、1~5個の任意のアミノ酸が欠失、置換若しくは付加したBNP-32のアミノ酸配列中の5アミノ酸以上の連続する任意のアミノ酸配列を含むペプチド、1~5個の任意のアミノ酸が欠失、置換若しくは付加したBNP-45のアミノ酸配列中の5アミノ酸以上の連続する任意のアミノ酸配列を含むペプチドからなる群より選択されるペプチドであり、
かつ、CNP活性またはBNP活性を有するキメラペプチド、あるいは、その誘導体を用いることが好ましい。
被験者の診断と評価。
まず、ナトリウム利尿ペプチド製剤の投与に先だって被験者の診断と評価を行った。被験者の診断と評価方法は下記のとおりである。
被験者は、円形脱毛症、男性型脱毛症、分娩後脱毛症、女性型脱毛症、批糠性脱毛症または老人性脱毛症の患者である。これら被験者の診断と処置は、本発明者が医師として実施した。
脱毛症の臨床的分類は日本皮膚科学会の分類に従い、円形脱毛症の重症度の評価は、前記の「米国の円形脱毛症評価ガイドライン」に従って、脱毛の範囲についてS0~S5の6段階および脱毛部位についてB0~B2の3段階に分類して行った。
一般に、個々の症例に対する外用薬の効果を確認するためには、左右塗り分け法が好適である。左右塗り分け法は、例えば、疾患部位の左側には試験すべき有効成分を含んだ外用薬を塗布し、右側には有効成分を含まない外用薬を塗布して、その治療効果を確認する方法である。本発明製剤の試験も、予備試験においては左右塗り分け法に従って行った。ただし、医療倫理に鑑み、左右塗り分け法による予備試験は最小限にとどめ、予備試験を行なわない場合には、塗布前と塗布後の比較により、治療効果を判定した。
1.ゲル剤の製造
NPを有効成分として含む軟膏剤(ワセリン製剤)の調製は、主剤として、ヒトANP(1-28)(株式会社ペプチド研究所製)、ヒトBNP-32(株式会社ペプチド研究所製)、ヒトCNP-22(株式会社ペプチド研究所製)のいずれかを3mg秤量し、これを3mlの生理食塩水に溶解して得られた1000μg/mlの濃度の各NP溶液1mlを9gの日本薬局方の白色ワセリンに高速撹拌で均一に混合し、撹拌することによって、100μg/g濃度のANP軟膏剤、BNP軟膏剤およびCNP軟膏剤を作製した。
BNPとベタメタゾンとゲンタマイシン合剤の調製は、岩城製薬株式会社製のデルモゾール(商標)Gローション(Dermosol-G Lotion)を上記「1.ゲル剤の製造」で得たBNPのゲル剤と等容量で混合することにより作製した。本明細書において、これをBNP:ベタメタゾン:ゲンタマイシン合剤と呼ぶ。デルモゾールGローションはベタメタゾン吉草酸エステルを1200μg/mlの濃度で含むとともに、ゲンタマイシン硫酸塩を1000μg/mlの濃度で含むことから、100μg/gの濃度のCNPゲル剤とデルモゾールGローションを1:1の容量比で混合することにより、50μg/gの濃度のCNPと、600μg/mlの濃度のベタメタゾン吉草酸エステルと、500μg/mlの濃度のゲンタマイシン硫酸塩を含有する合剤を作製した。本明細書において、これを50μg/gBNP:600μg/mlベタメタゾン:500μg/mlゲンタマイシン合剤と呼ぶ。
CNPとベタメタゾンとゲンタマイシン合剤の調製は、岩城製薬株式会社製のデルモゾール(商標)Gローション(Dermosol-G Lotion)を上記「1.ゲル剤の製造」で得たCNPのゲル剤と等容量で混合することにより作製した。本明細書において、これをCNP:ベタメタゾン:ゲンタマイシン合剤と呼ぶ。デルモゾールGローションはベタメタゾン吉草酸エステルを1200μg/mlの濃度で含むとともに、ゲンタマイシン硫酸塩を1000μg/mlの濃度で含むことから、100μg/gの濃度のCNPゲル剤とデルモゾールGローションを1:1の容量比で混合することにより、50μg/gの濃度のCNPと、600μg/mlの濃度のベタメタゾン吉草酸エステルと、500μg/mlの濃度のゲンタマイシン硫酸塩を含有する合剤を作製した。本明細書において、これを50μg/gCNP:600μg/mlベタメタゾン:500μg/mlゲンタマイシン合剤と呼ぶ。
BNPとクロベタゾールプロピオン酸エステルとの合剤の調製は、グラクソ・スミスクライン株式会社製のデルモベート(商標)スカルプローション0.05%(Dermovate Scalp Lotion 0.05%)を上記「1.ゲル剤の製造」で得たBNPのゲル剤と等容量で混合することにより作製した。本明細書において、これをBNP:クロベタゾール合剤と呼ぶ。デルモベートスカルプローション0.05%はクロベタゾールプロピオン酸エステルを500μg/gの濃度で含むことから、100μg/mlの濃度のBNPゲル剤とデルモベートスカルプローション0.05%を1:1の容量比で混合することにより、50μg/mlの濃度のBNPと250μg/gの濃度のクロベタゾールプロピオン酸エステルを含有する合剤を作製した。本明細書において、これを50μg/mlBNP:250μg/gクロベタゾール合剤と呼ぶ。
CNPとクロベタゾールプロピオン酸エステルとの合剤の調製は、グラクソ・スミスクライン株式会社製のデルモベート(商標)スカルプローション0.05%(Dermovate Scalp Lotion 0.05%)を上記「1.ゲル剤の製造」で得たCNPのゲル剤と等容量で混合することにより作製した。本明細書において、これをCNP:クロベタゾール合剤と呼ぶ。デルモベートスカルプローション0.05%はクロベタゾールプロピオン酸エステルを500μg/gの濃度で含むことから、100μg/mlの濃度のCNPゲル剤とデルモベートスカルプローション0.05%を1:1の容量比で混合することにより、50μg/mlの濃度のCNPと250μg/gの濃度のクロベタゾールプロピオン酸エステルを含有する合剤を作製した。本明細書において、これを50μg/mlCNP:250μg/gクロベタゾール合剤と呼ぶ。
CNPと塩化カルプロニウムとの合剤の調製は、大洋薬品工業株式会社製のカルプラニン(商標)外用液5%(CALPRANIN)を上記「1.ゲル剤の製造」で得たCNPのゲル剤と等容量で混合することにより作製した。本明細書において、これをCNP:塩化カルプロニウム合剤と呼ぶ。カルプラニン外用液5%は塩化カルプロニウムを50mg/mlの濃度で含むことから、100μg/mlの濃度のCNPゲル剤とカルプラニン外用液5%を1:1の容量比で混合することにより、50μg/mlの濃度のCNPと50mg/mlの濃度の塩化カルプロニウムを含有する合剤を作製した。本明細書において、これを50μg/mlCNPゲル剤:50mg/ml塩化カルプロニウム合剤と呼ぶ。
1.被験者の診断および治療
本発明のANPゲル剤、BNPゲル剤、CNPゲル剤、BNP軟膏剤およびCNP軟膏剤の投与に先だって、皮膚科診療におけるルーチンとして、被験者への性別、年齢、病歴、家族歴の問診、アレルギー体質が疑われる場合には、主要なアレルゲンに対するスクラッチ(Scratch)試験、および、それらの評価を行った。なお、皮膚科診療においては、特定のアレルゲンに対する強い免疫反応性を有する患者や、アトピー性皮膚炎などのアレルギー素因の疑われる疾患が比較的多いことから、診断を補助する目的で、性別、年齢に加えて、アレルギー性疾患の家族歴および既往歴の問診および主要なアレルゲンに対するスクラッチ(Scratch)試験を行なうことは、簡便な補助検査法として、広く行なわれている。
スクラッチ(Scratch)試験の結果の評価としては、いずれかのアレルゲンに1+以上の反応性を示せば、多少であってもアレルギー体質を有するということができる。但し、皮膚科に来院する患者の場合、スクラッチ(Scratch)試験を行なえば、何らかのアレルゲンに対しては1+または2+の反応性を示すことが多く、全てのアレルゲンに対して全く反応性を示さない患者は少ない。スクラッチ(Scratch)試験はアレルギー体質の有無についての目安を得るための簡易検査であるので、その結果を持ってアレルギー体質の有無を正確に評価することはできないが、経験的には、特定のアレルゲンに対して2+以上の反応性を示す場合には、診断に際して免疫性疾患との関連に留意する。
表1~表23に、それら被験者への問診結果、、スクラッチ(Scratch)試験結果を、前記の〔実施例1〕で行なった、被験者の診断所見および症状の評価とともに示す。
円形脱毛症に対する治療効果:
ANP: 表1、表2
BNP: 表3-1、表3-2
CNP: 表4、表5、表6、表7-1
BNP:ベタメタゾン:ゲンタマイシン合剤: 表7-2
CNP:ベタメタゾン:ゲンタマイシン合剤: 表7-3
男性型脱毛症に対する治療効果:
ANP: 表8
BNP: 表9-1、表9-2
CNP: 表10-1、表10-2
CNP:ベタメタゾン:ゲンタマイシン合剤: 表10-3
CNP:クロベタゾール合剤: 表10-4
CNP:塩化カルプロニウム合剤: 表10-5
CNPゲル剤とミノキシジルの重層塗布: 表10-6
BNPゲル剤とミノキシジルの重層塗布: 表10-7
分娩後脱毛症に対する治療効果:
ANP: 表10-8
BNP: 表10-9
CNP: 表11-1
女性型脱毛症に対する治療効果:
BNP: 表11-2
CNP: 表12
脂漏性脱毛症に対する治療効果:
ANP: 表13
BNP: 表14
批糠性脱毛症に対する治療効果:
ANP: 表15
BNP: 表16
CNP: 表17、表18
老人性脱毛症に対する治療効果:
ANP: 表19
BNP: 表20
CNP: 表21
癌化学療法剤性脱毛症に対する治療効果:
BNP: 表22
CNP: 表23
2.ANPゲル剤の円形脱毛症に対する治療効果
ANPゲル剤の円形脱毛症に対する治療効果を表1(症例A1~A5)および表2(症例A6~A7)に示す。

被験者は33歳の女性であり、脱毛範囲はS3で、頭部以外に眉毛の脱毛を伴うB1の重症の円形脱毛症患者である。アトピー性皮膚炎の既往歴があり、アトピー性皮膚炎の悪化にともなって出現した脱毛症も合併している。スクラッチテストの結果は、ハウスダスト2+、ダニ1+、カモガヤ2+、ブタクサ2+であった。この被験者は、脱毛部位の頭皮に、掻痒を伴う粃糠様鱗屑と紅班がみられ、批糠性脱毛症を合併している。この被験者は、13歳で円形脱毛班が出現し、14歳の時に頭頂部にも出現後、半月で全頭脱毛症になった。その後、この被験者の症状は一進一退で15歳で全身の脱毛症になった。この被験者は、ステロイドの外用と内服では全く治療効果が見られなかった。この被験者は、液体窒素の刺激療法を続けていたが、全くと言ってよいほど治療効果はみられなかった。尚、この被験者は、症例C5と同じ被験者である。
被験者は33歳の女性であり、脱毛範囲はS3の重症の円形脱毛症患者である。スクラッチテストの結果は、ハウスダスト2+、ダニ3+、スギ3+、カモガヤ2+、ブタクサ2+であった。この被験者は、2年前にも円形脱毛症に罹患し2カ所脱毛巣ができたことがあったが、自然治癒した。今回は半年前に職場のストレスが1ヶ月位つづいた後、右側頭部、後頭部および頭頂部に脱毛班が出現した。この被験者は、6ヶ月間ステロイドの外用、塩化カルプロニウムの塗布、セファランチン内服での治療をうけるも、なんの変化もみられなかった。
被験者は52歳の女性であり、脱毛範囲はS3の重症の円形脱毛症患者である。アレルギー性鼻炎の既往歴がある。スクラッチテストの結果は、ハウスダスト1+、スギ2+、カモガヤ1+、ブタクサ1+であった。この被験者は、夜勤が続いていて1年位前に前頭部に脱毛巣が出現し、その後拡大傾向をしめし、頭皮全体にも脱毛班が出現し多発してきた。脱毛巣への塩化カルプロニウムの塗布を8ヶ月間続けたが、脱毛範囲が広がる一方で全く治療効果はみられなかった。この被験者は、脱毛部の頭皮に紅班、痂皮、鱗屑等の炎症症状は見られない症例である。尚、この被験者は、症例C15の被験者と同じ被験者である。
被験者は32歳の男性であり、脱毛範囲はS1の円形脱毛症患者である。アトピー性皮膚炎とアレルギー性鼻炎の既往歴がある。スクラッチテストの結果は、ハウスダスト2+、ダニ3+、スギ2+、カモガヤ2+、ブタクサ2+であった。この被験者は、1ヶ月前より精神的ストレスが引き金となり左側頭部に脱毛班が出現し、その後頭頂部、右側頭部にも脱毛班がみられるようになった。掻痒を伴った。
被験者は16歳の男性であり、脱毛範囲はS3で、難治といわれる蛇行状脱毛症型の円形脱毛症患者である。この被験者はアトピー性皮膚炎を合併している。スクラッチテストの結果は、ハウスダスト3+、ダニ3+、カモガヤ2+、ブタクサ1+であった。この被験者は、6歳でアデノイドと口蓋扁桃摘出手術をしたのち、7歳から円形脱毛症を発症し、頭部の他、眉毛、下肢の脱毛がみられた。この被験者は、ステロイドの内服、外用でも治癒しなかった。この被験者の脱毛部位の頭皮は浸潤性紅班、鱗屑がみられ掻痒を伴っていた。尚、この被験者は、症例B3の被験者と同一の被験者である。

被験者は50歳の女性であり、脱毛範囲はS2で、多発性脱毛症の重症の円形脱毛症患者である。アトピー性皮膚炎とアレルギー性鼻炎の既往歴がある。本人の母に円形脱毛症の既往があり、子供はアレルギー性鼻炎と慢性蕁麻疹に罹患している。スクラッチテストの結果は、ハウスダスト1+、ダニ1+、カモガヤ2+、ブタクサ1+であった。この被験者は、脱毛部位の頭皮に、掻痒を伴う粃糠様鱗屑と紅班がみられ、批糠性脱毛症を合併している。この被験者は、10年前に多発性の円形脱毛症を発症し、円形脱毛症の部分寛解と再燃を繰り返している。この被験者は、仕事が多忙になると脱毛症状が増悪する傾向をしめす。ステロイドと塩化カルプロニウム外用や、抗アレルギー剤の内服を6ヶ月間行うも効果が見られなかった。尚、この被験者は、症例C3および症例C4の被験者と同一の被験者である。
この被験者の頭頂部の多発性脱毛班に100μg/gのANPゲル剤を2週間塗布したが効果はなく、かさかさした鱗屑が増加し、紅班が出現し、掻痒を生じ、抜け毛もふえ、脱毛範囲がむしろ拡大してしまった(図11を参照)。
被験者は22歳の女性であり、脱毛範囲はS3で、難治性といわれる蛇行状脱毛症型の円形脱毛症の重症患者である。この被験者は、アトピー性皮膚炎とアレルギー性鼻炎の既往歴がある。この被験者の祖父がアトピー性皮膚炎、父、母、兄はアレルギー性鼻炎に罹患している。スクラッチテストの結果は、ハウスダスト2+、ダニ3+、カモガヤ1+であった。この被験者は、1年半以上前に脱毛班が発症し、全く発毛しない状態で被髪部外側縁に沿って境界鮮明に帯状に脱毛班がみられた。この被験者の脱毛部位に紅班、鱗屑、痂皮、およびアトピー性脱毛症によるとおもわれる炎症症状がみられ、掻痒を伴っていた。この被験者は、頭部の他、眉毛にも脱毛がみられた。この被験者の皮膚はステロイドのリバウンドによると思われる紅皮症状態であり、頭皮も含む全身の皮膚に潮紅、浸潤がみられた。この被験者は、ステロイド、抗アレルギー剤の治療では全く治療効果がなかった。尚、この被験者は、症例C6の被験者と同じ被験者である。
BNPゲル剤の治療効果を表3-1(症例B1~B4およびB13)および表3-2(症例B26)に示す。

被験者は63歳の女性であり、脱毛範囲はS2で、多発性円形脱毛症の重症患者である。この被験者は、アレルギ-性鼻炎の既往があり、アトピー性皮膚炎を合併している。スクラッチテストの結果は、ハウスダスト2+、ダニ1+、カモガヤ2+、ブタクサ1+であった。この被験者の円形脱毛症は、1年半以上持続している。この被験者は、以前、脱毛班にステロイドと塩化カルプロニウムを10ヶ月塗布し続けたが効果がなく発毛はみられなかった。尚、この被験者は、症例C12の被験者と同じ被験者である。
被験者は13歳の男性であり、脱毛範囲はS1の単発性円形脱毛症である。この被験者にスクラッチテストは行っていない。
被験者は16歳の男性であり、脱毛範囲はS3で、難治といわれる蛇行状脱毛症型の円形脱毛症患者である。アトピー性皮膚炎を合併している。スクラッチテストの結果は、ハウスダスト3+、ダニ3+、カモガヤ2+、ブタクサ1+であった。この被験者は、6歳でアデノイドと口蓋扁桃摘出手術をしたのち、7歳から円形脱毛症を発症し、頭部の他、眉毛、下肢の脱毛がみられた。この被験者は、ステロイドの内服、外用でも治癒しなかった。この被験者の脱毛部位の頭皮は浸潤性紅班、鱗屑がみられ掻痒を伴っていた。尚、この被験者は、症例A5の被験者と同一の被験者である。
この被験者は、その後、来院しておらず、その後の経過は不明である。
被験者は24歳の女性であり、脱毛範囲はS2で、多発性円形脱毛症の重症患者である。アレルギー性鼻炎の既往がある。母が気管支喘息に罹患している。スクラッチテストの結果は、ハウスダスト2+、ダニ2+、スギ2+、カモガヤ1+、ブタクサ1+であった。この被験者の円形脱毛症は、中学生の時から部分寛解と再燃をくりかえしていた。半年前から前頭部を中心に軽度の掻痒感が出現し、その後多発性の脱毛班が拡大した。この被験者は、ステロイドや塩化カルプロニウムを3ヶ月間の脱毛部位へ塗布しても、抗アレルギー剤を内服しても発毛がみられず、易脱毛性も改善されなかった。尚、この被験者は、症例C9の被験者と同一の被験者である。
被験者は39歳の男性であり、後述するC13の症例の被験者と同じ被験者である。この被験者の側頭部および後頭部の円形脱毛班は、100μg/gのCNP軟膏剤を1日2回塗布したところ、1週間の塗布で発毛し、1週間で塗布中止した後に自然に治癒した。しかし、CNP軟膏剤の塗付中止から10ヶ月経過後に、今度は頭頂部に円形脱毛班が生じた。
BNP軟膏剤の治療効果を表3-2(被験者B5、B6)に示す。

被験者は50歳の女性であり、脱毛範囲はS3で、多発性円形脱毛症の重症患者である。アレルギ-性鼻炎の既往があり、アトピー性皮膚炎を合併している。スクラッチテストの結果は、ハウスダスト3+、ダニ3+、スギ3+、カモガヤ2+、ブタクサ2+であった。この被験者の円形脱毛症は、4ヶ月前から職場の人間関係によるストレスで発症し、発症から2ヶ月後には多発しはじめた。この被験者は、脱毛部位にステロイドステロイドローションと塩化カルプロニウムを10ヶ月間塗布し続けたが、発毛はみられず、易脱毛性も抑制されず、治療効果がなかった。
被験者は33歳の女性であり、脱毛範囲はS1の円形脱毛症患者である。この被験者の子供はアトピー性皮膚炎に罹患している。この被験者の母は、円形脱毛症であるとともに、アレルギー性鼻炎の既往がある。スクラッチテストの結果は、ハウスダスト2+、ダニ2+、カモガヤ2+、ブタクサ2+であり、アトピー素因を持った症例であった。この被験者は、5ヶ月前に円形脱毛班が出現し、ステロイドの外用、塩化カルプロニウムの塗布、抗アレルギー剤の内服による治療を7週間続けるも、抜け毛がおさまらないだけでなく脱毛範囲が拡大し多発したためステロイドの内服も併用したが、治療効果はみられなかった。この被験者は、左側頭部、頭頂部、後頭部に脱毛班がみられ、脱毛範囲はS1であった。尚、この被験者は、症例C10の被験者と同じ被験者である。
被験者は38歳の女性であり、脱毛範囲はS1の単発性円形脱毛症患者である。この被験者の子供がアトピー性皮膚炎に罹患している。この被験者は、従兄弟、姪、叔母子供も多発性円形脱毛症に罹患している。この被験者にスクラッチテストは行っていない。
そこで、50μg/gのBNPゲル剤を1日2回、2週間塗布したところ、顕著に発毛して硬毛化し、ほぼ治癒した(図55)。BNPゲル剤の塗付を2週間で終了し、その後6週間経過したが、完治して再燃じていない(図55)。
尚、この被験者は、症例C7の被験者と同一の被験者である。
CNPゲル剤の円形脱毛症に対する治療効果を表4(被験者C1、C3、C20、C23)に示す。
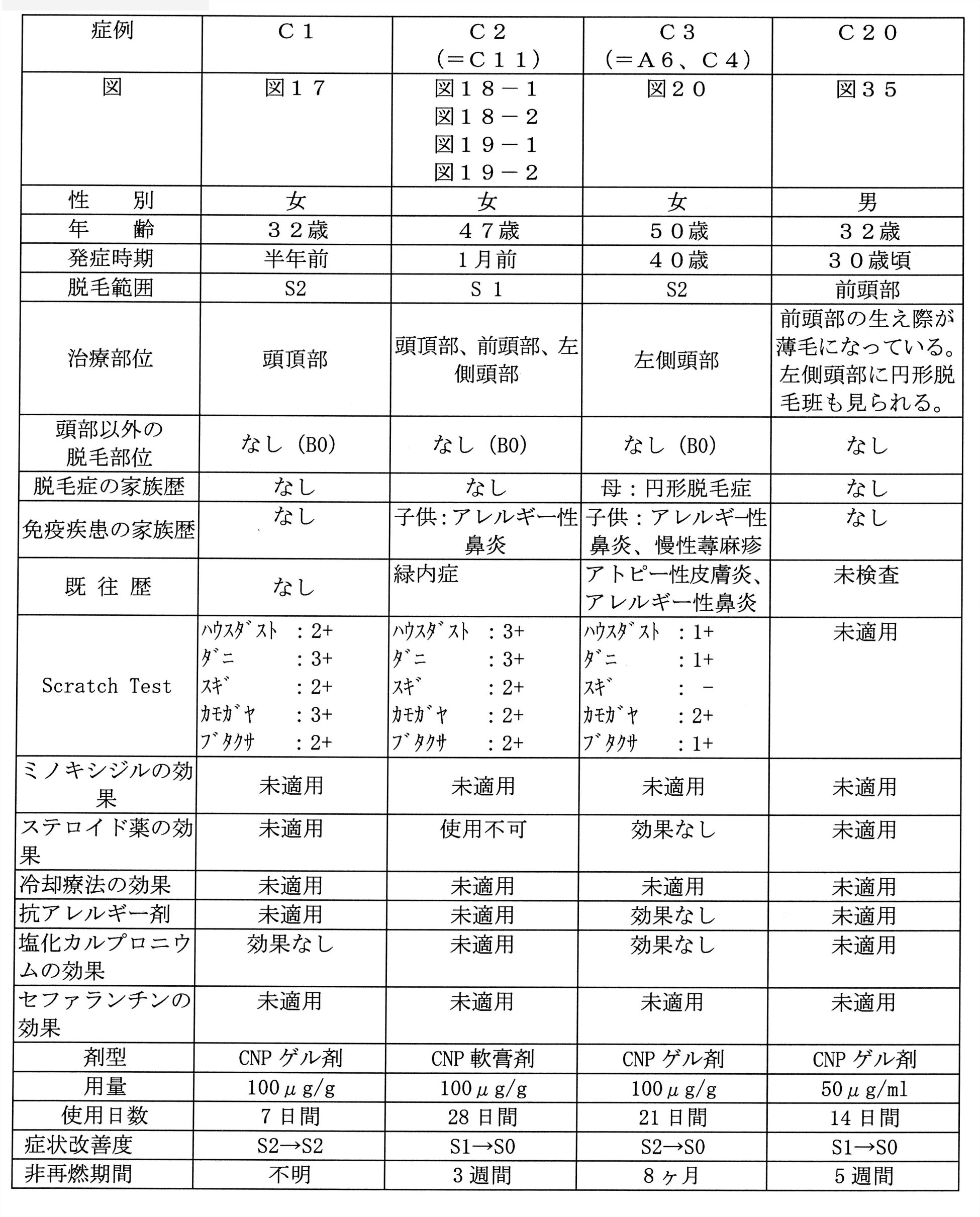
被験者は32歳の女性であり、脱毛範囲はS3で、多発性円形脱毛症の重症患者である。アレルギ-性鼻炎の既往がある。スクラッチテストの結果は、ハウスダスト2+、ダニ3+、スギ2+、カモガヤ3+、ブタクサ2+であった。この被験者の円形脱毛症は、半年前に脱毛症が発症し、拡大、多発するとともに発症の5ヶ月後には頭皮全体に脱毛傾向がみられるようになった。この被験者は、職場が変わったことが円形脱毛症発症の引き金になった。この被験者は、塩化カルプロニウムの塗布では治療効果が見られなかった。
被験者は47歳の女性であり、脱毛範囲はS1の円形脱毛症患者である。この被験者は、緑内障の既往歴がある。この被験者の子供はアトピー性皮膚炎とアレルギー性鼻炎に罹患している。スクラッチテストの結果は、ハウスダスト3+、ダニ3+、スギ2+、カモガヤ2+、ブタクサ2+であった。この被験者は、1ヶ月前に脱毛巣が頭頂部に出現し、その後、前頭部および左側頭部にも脱毛班がみられるようになった。この被験者は、緑内障の既往があるためステロイドの使用は避けなければならない症例である。この被験者は、7年前に甲状腺癌に罹患し、摘出手術を受けている。尚、この被験者は、症例C11の被験者と同じ被験者である。
被験者は50歳の女性であり、脱毛範囲はS2で、多発性円形脱毛症の重症患者である。この被験者は、アトピー性皮膚炎とアレルギー性鼻炎の既往歴がある。この被験者の母が円形脱毛症の既往があり、子供はアレルギー性鼻炎と慢性蕁麻疹に罹患している。スクラッチテストの結果は、ハウスダスト1+、ダニ1+、カモガヤ2+、ブタクサ1+であった。この被験者は、脱毛部位の頭皮に、掻痒を伴う粃糠様鱗屑と紅班がみられ、批糠性脱毛症の合併している。この被験者は、10年前に多発性の円形脱毛症が発症し、部分寛解と再燃を繰り返している。この被験者の場合、仕事が多忙になると円形脱毛症の増悪傾向をしめす。ステロイド外用、塩化カルプロニウム外用、および、抗アレルギー剤の内服を6ヶ月間行うも効果が見られなかった。尚、この被験者は、症例A6および症例C4の被験者と同一の被験者である。
被験者は32歳の男性で、男性型脱毛症である。この被験者は、30歳になって急に前頭部のM型部の生え際が薄毛になって後退した。また、来院の6週間前に左側頭部に単発性の円形脱毛症も発症した。この被験者の家族に脱毛症患者はいない。この被験者は、Hamilton-Norwood分類ではIII型に属する、いわゆるM型の男性型脱毛症である。尚、この被験者は、症例C27の被験者と同じ被験者である。
CNP軟膏剤の円形脱毛症に対する治療効果を表4(症例C2)、表5(被験者C4~C7)、表6(被験者C8~C12)および表7-1(被験者C13~C15、C36)に示す。
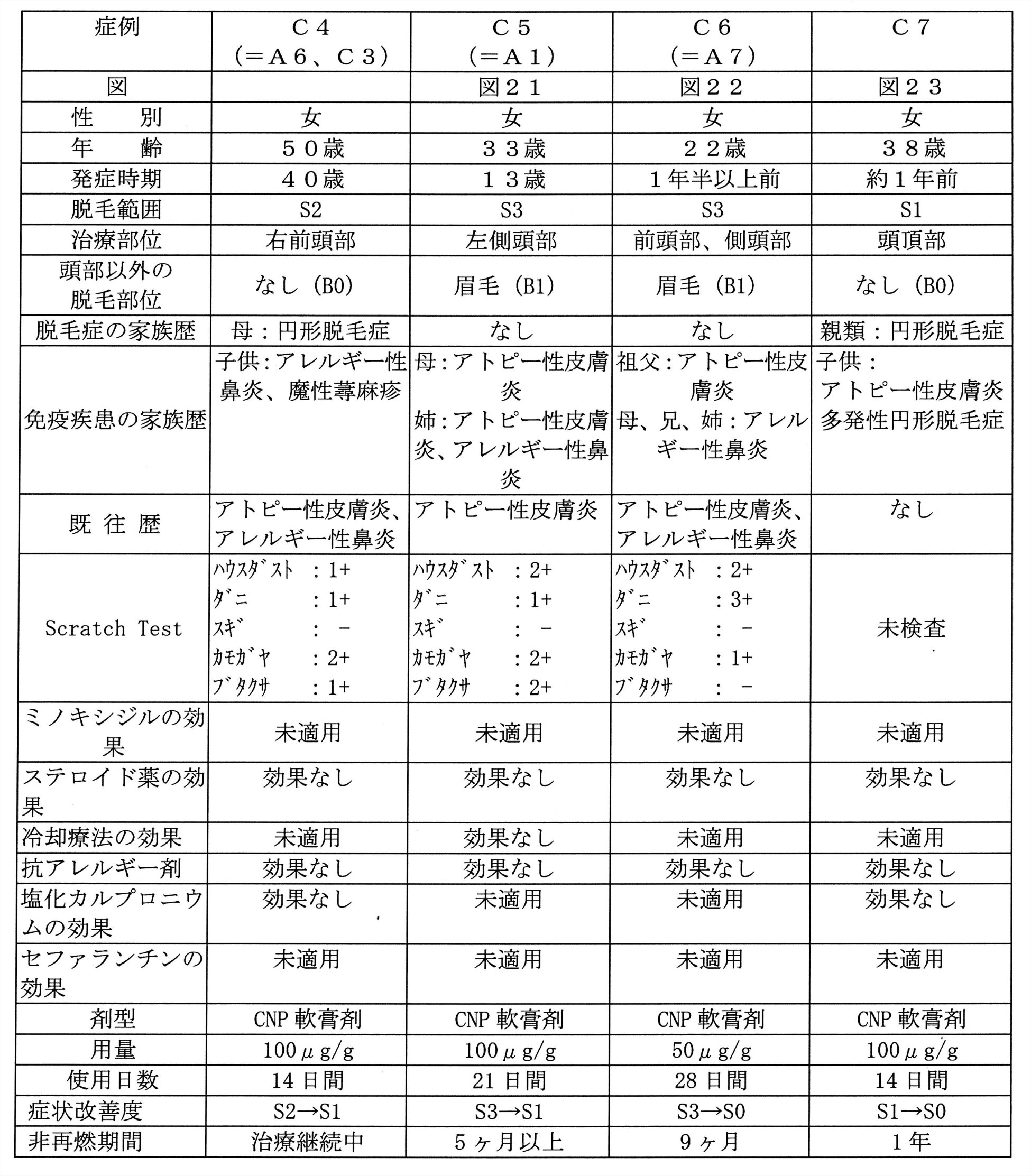
被験者は50歳の女性であり、脱毛範囲はS2で、多発性円形脱毛症の重症患者である。この被験者は、アトピー性皮膚炎とアレルギー性鼻炎の既往歴がある。この被験者の母が円形脱毛症の既往があり、子供はアレルギー性鼻炎と慢性蕁麻疹に罹患している。スクラッチテストの結果は、ハウスダスト1+、ダニ1+、カモガヤ2+、ブタクサ1+であった。この被験者は、脱毛部位の頭皮に、掻痒を伴う粃糠様鱗屑と紅班がみられ、批糠性脱毛症の合併している。この被験者は、10年前に多発性の円形脱毛症が発症し、部分寛解と再燃を繰り返している。この被験者の場合、仕事が多忙になると円形脱毛症の増悪傾向をしめす。ステロイド外用、塩化カルプロニウム外用、および、抗アレルギー剤の内服を6ヶ月間行うも効果が見られなかった。尚、この被験者は、症例A6および症例C3の被験者と同一の被験者である。
被験者は33歳の女性であり、脱毛範囲はS3で、頭部以外に眉毛の脱毛を伴うB1の円形脱毛症の重症患者である。アトピー性皮膚炎の既往歴があり、アトピー性皮膚炎の悪化による脱毛症も合併している。スクラッチテストの結果は、ハウスダスト2+、ダニ1+、カモガヤ2+、ブタクサ2+であった。この被験者は、脱毛部位の頭皮に、掻痒を伴う粃糠様鱗屑と紅班がみられ、批糠性脱毛症の合併している。この被験者は、13歳で円形脱毛班が出現し、14歳の時頭頂部にも出現後、半月で全頭脱毛症になった。その後、この被験者の症状は一進一退で15歳で、全身の脱毛症になった。この被験者は、ステロイドの外用と内服では全く治療効果が見られなかった。この被験者は、液体窒素の刺激療法を続けていたが全くと言ってよいほど治療効果はみられなかった。尚、この被験者は、症例A1の被験者と同一の被験者である。
被験者は22歳の女性であり、脱毛範囲はS3で、難治性といわれる蛇行状脱毛症型の円形脱毛症の重症患者である。この被験者は、アトピー性皮膚炎とアレルギー性鼻炎の既往歴がある。この被験者の祖父がアトピー性皮膚炎、父、母、兄はアレルギー性鼻炎に罹患している。スクラッチテストの結果は、ハウスダスト2+、ダニ3+、カモガヤ1+であった。この被験者は、1年半以上前に脱毛班が発症し、全く発毛しない状態で被髪部外側縁に沿って境界鮮明に帯状に脱毛班がみられた。この被験者の脱毛部位に紅班、鱗屑、痂皮が見られ、アトピー性脱毛症によるとおもわれる炎症症状がみられ、掻痒を伴っていた。この被験者は、頭部の他、眉毛にも脱毛がみられた。この被験者は、アトピー性皮膚炎とアレルギー性鼻炎の合併症例である。この被験者の皮膚は、ステロイドのリバウンドによると思われる紅皮症状態であり、頭皮も含む全身の皮膚に潮紅、浸潤がみられた。この被験者は、ステロイド、抗アレルギー剤の治療では全く治療効果がなかった。尚、この被験者は、症例A7の被験者と同じ被験者である。
被験者は38歳の女性であり、脱毛範囲はS1の単発性円形脱毛症患者である。この被験者の子供がアトピー性皮膚炎に罹患している。この被験者は、従兄弟、姪、叔母子供も多発性円形脱毛症に罹患している。この被験者にスクラッチテストは行っていない。
そこで、50μg/gのBNPゲル剤を1日2回、2週間塗布したところ、顕著に発毛して硬毛化し、ほぼ治癒した。
尚、この被験者は、症例B26の被験者と同一の被験者である。

被験者は32歳の女性であり、脱毛範囲はS1の多発性円形脱毛症患者である。スクラッチテストの結果は、ハウスダスト-、ダニ1+、スギ2+、カモガヤ2+、ブタクサ2+であった。この被験者は、1年半前に多発性脱毛症に罹患し、1年半前にわたって、ステロイドの外用、塩化カルプロニウムの塗布、抗アレルギー剤の内服による治療を続けるも、満足のゆく効果は得られなかった。この被験者の脱毛部には軽度の紅班がみられ、掻痒感を伴っていた。この被験者の場合、右側頭部、左側頭部に脱毛班が多発していた。
被験者は24歳の女性であり、脱毛範囲はS2で、多発性円形脱毛症の重症患者である。アレルギー性鼻炎の既往がある。母が気管支喘息に罹患している。スクラッチテストの結果は、ハウスダスト2+、ダニ2+、スギ2+、カモガヤ1+、ブタクサ1+であった。この被験者の円形脱毛症は、中学生の時から部分寛解と再燃をくりかえしていた。半年前から前頭部を中心に軽度の掻痒感が出現し、その後多発性の脱毛班が拡大した。この被験者は、ステロイドや塩化カルプロニウムを3ヶ月間の脱毛部位へ塗布しても、抗アレルギー剤を内服しても発毛がみられず、易脱毛性も改善されなかった。尚、この被験者は、症例B4の被験者と同じ被験者である。
被験者は33歳の女性であり、脱毛範囲はS1の円形脱毛症患者である。この被験者の子供はアトピー性皮膚炎に罹患している。この被験者の母は、円形脱毛症であるとともに、アレルギー性鼻炎の既往がある。スクラッチテストの結果は、ハウスダスト2+、ダニ2+、カモガヤ2+、ブタクサ2+であり、アトピー素因を持った症例であった。この被験者は、5ヶ月前に円形脱毛班が出現し、ステロイドの外用、塩化カルプロニウムの塗布、抗アレルギー剤の内服による治療を7週間続けるも、抜け毛がおさまらないだけでなく脱毛範囲が拡大し多発したためステロイドの内服も併用したが、治療効果はみられなかった。この被験者は、左側頭部、頭頂部、後頭部に脱毛班がみられ、脱毛範囲はS1であった。尚、この被験者は、症例B6の被験者と同じ被験者である。
被験者は47歳の女性であり、脱毛範囲はS1の円形脱毛症患者である。この被験者は、緑内障の既往歴がある。この被験者の子供はアトピー性皮膚炎とアレルギー性鼻炎に罹患している。スクラッチテストの結果は、ハウスダスト3+、ダニ3+、スギ2+、カモガヤ2+、ブタクサ2+であった。この被験者は、1ヶ月前に脱毛巣が頭頂部に出現し、その後、前頭部および左側頭部にも脱毛班がみられるようになった。この被験者は、緑内障の既往があるためステロイドの使用は避けなければならない症例である。この被験者は、7年前に甲状腺癌に罹患し、摘出手術を受けている。尚、この被験者は、症例C2の被験者と同じ被験者である。

被験者は63歳の女性であり、脱毛範囲はS2で、多発性円形脱毛症の重症患者である。アレルギー性鼻炎の既往があり、アトピー性皮膚炎を合併している。スクラッチテストの結果は、ハウスダスト2+、ダニ1+、カモガヤ2+、ブタクサ1+であった。この被験者の円形脱毛症は、1年半以上持続している。この被験者は、脱毛班にステロイドと塩化カルプロニウムを10ヶ月塗布し続けたが効果がなく発毛はみられなかった。尚、この被験者は、症例B1の被験者と同じ被験者である。
被験者は38歳の男性であり、脱毛範囲はS1で、多発性円形脱毛症の患者である。2ヶ月前より脱毛巣が側頭部に出現し、その後後頭部にも脱毛班がみられるようになった。免疫疾患の既往または家族歴はない。この被験者のスクラッチテストの結果は、ハウスダスト2+、ダニ2+、スギ2+、カモガヤ2+、ブタクサ1+であった。この被験者は、セファランチンの内服をしたが治療効果はみられなかった。
被験者は35歳の女性であり、脱毛範囲はS1の円形脱毛症患者であるである。この被験者はアレルギー性鼻炎の既往があり、この被験者の母親もアレルギー性鼻炎に罹患しており、この被験者はアトピー素因を持っている症例である。この被験者のスクラッチテストの結果は、ハウスダスト2+、ダニ2+、スギ2+、カモガヤ2+、ブタクサ1+であった。この被験者は、3ヶ月前に後頭部に脱毛巣が出現し、その後拡大傾向をしめし、後頭部全体が薄くなってきて掻痒を伴っていた。この被験者の場合、ステロイド剤の塗布では痒くなって、かえって脱毛範囲が広がってしまった。
被験者は52歳の女性であり、脱毛範囲はS3の重症の円形脱毛症患者である。アレルギー性鼻炎の既往歴がある。スクラッチテストの結果は、ハウスダスト1+、スギ2+、カモガヤ1+、ブタクサ1+であった。この被験者は、夜勤が続いていて1年位前に前頭部に脱毛巣が出現し、その後拡大傾向をしめし、頭皮全体にも脱毛班が出現し多発してきた。脱毛巣への塩化カルプロニウムの塗布を8ヶ月間続けたが、脱毛範囲が広がる一方で全く治療効果はみられなかった。この被験者は、脱毛部の頭皮に紅班、痂皮、鱗屑等の炎症症状は見られない症例である。尚、この被験者は、症例A3の被験者と同じ被験者である。
被験者は57歳の男性であり、脱毛範囲はS2で眉毛の脱毛も合併している重症の円形脱毛症患者である。この被験者は、アトピー性皮膚炎の既往歴がある。スクラッチテストの結果は、ハウスダスト1+、ダニ3+、スギ2+、カモガヤ1+、ブタクサ1+であった。この被験者は、仕事のストレスが原因で5年位前に脱毛巣が多発してきた。この被験者は、液体窒素療法を続けたが、脱毛範囲が広がる一方で全く治療効果はみられなかった。その後に、この被験者は、ステロイドの内服と外用、塩化カルプロニウム外用を3年にわたって行ったが効果はみられなかった。
被験者は26歳の女性であり、脱毛範囲はS1の単発性の円形脱毛症患者である。この被験者に脱毛症の既往歴はなく、この被験者の家族に円形脱毛症患者はいない。この被験者は、後頭部に単発性の円形脱毛症を発症して、他のクリニックを受診し、1.2mg/gのベタメタゾン吉草酸エステルを含有する、リンデロン(商標)-V軟膏(塩野義製薬株式会社)を6週間塗布したところ、少しだけ発毛したとのことであるが、脱毛班の大きさは拡大した。
BNP:ベタメタゾン:ゲンタマイシン合剤の円形脱毛症に対する治療効果を表7-2(症例B14)に示す。

被験者は31歳の女性であり、脱毛範囲はS1の単発性の円形脱毛症患者である。この被験者に円形脱毛症の家族はいない。この被験者のスクラッチテストの結果は、ハウスダスト-、ダニ1+、スギ1+、カモガヤ1+、ブタクサ2+であった。10年前にも多発性円形脱毛症に罹患したことがある。今回は、仕事が多忙だった時期に、頭頂部に単発性の円形脱毛症が発症した。
CNP:ベタメタゾン:ゲンタマイシン合剤の円形脱毛症に対する治療効果を表7-3(症例C21~C22)に示す。

被験者は51歳の男性であり、脱毛範囲はS1の単発性の円形脱毛症患者である。この被験者は、過去に円形脱毛症に罹患したことはなく、この被験者の家族にも円形脱毛症患者はいない。この被験者は、来院の約2ヶ月前から右頭頂部に単発性の円形脱毛班が出現した。
被験者は33歳の女性であり、頭頂部に単発性の円形脱毛班が出現して来院した。この被験者の脱毛範囲はS1の単発性の円形脱毛症患者である。この被験者の家族に円形脱毛症患者はいない。この被験者のスクラッチテストの結果は、ハウスダスト2+、ダニ1+、スギ3+、カモガヤ2+、ブタクサ2+であった。この被験者は、小学生と中学生のときにも円形脱毛症に罹患している。
ANPゲル剤の男性型脱毛症に対する治療効果を表8(症例A8~A9)に示す。
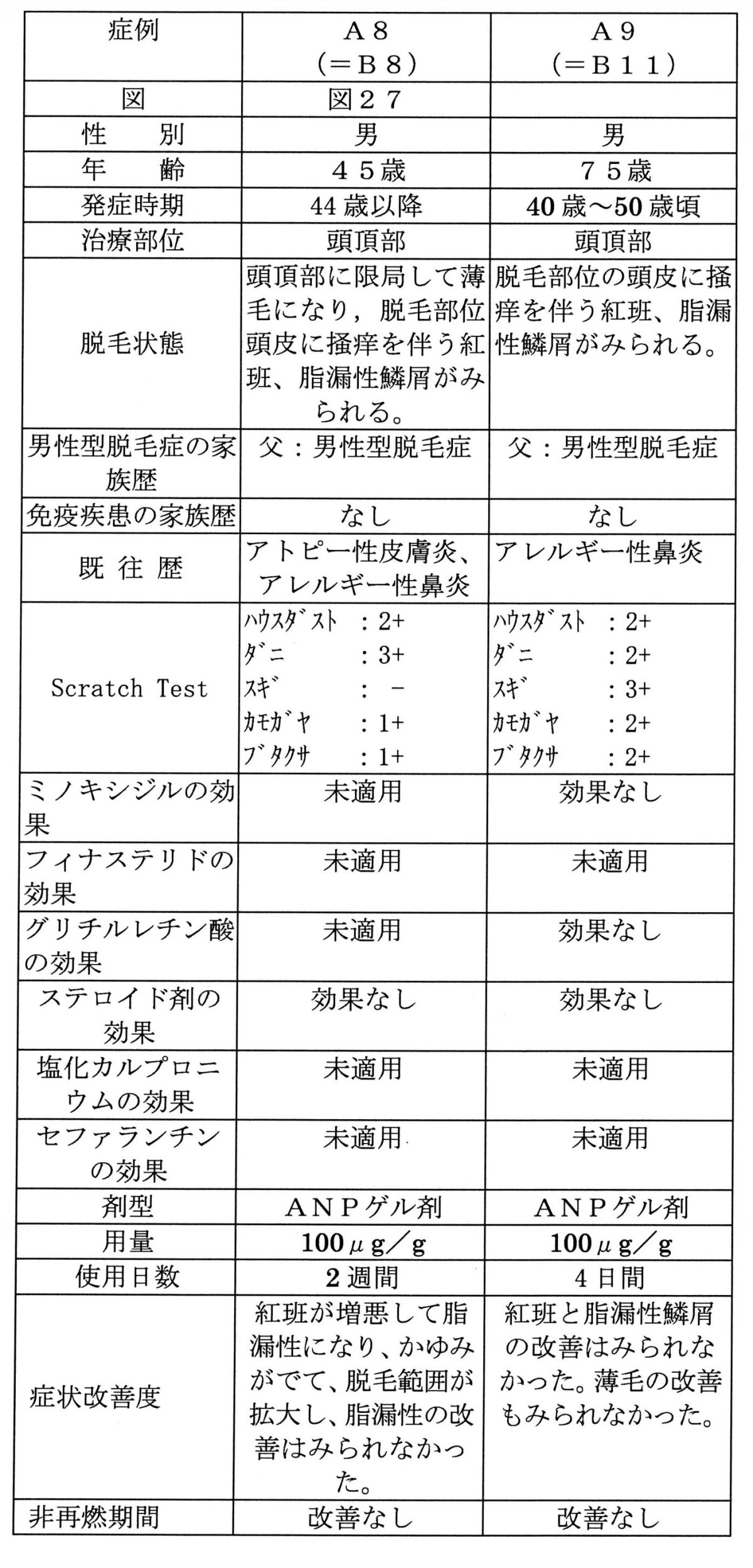
被験者は45歳の男性で、44歳頃から頭頂部に限局して薄毛になった。この被験者は、脱毛部位頭皮に掻痒を伴う紅班、脂漏性鱗屑がみられる、脂漏性脱毛症を合併している被験者である。Hamilton-Norwood分類ではIIvertex型に属する。この被験者の父は、頭頂部に限局した男性型脱毛症である。この被験者のスクラッチテストは、ハウスダスト2+、ダニ3+、カモガヤ1+、ブタクサ1+であった。この被験者は、症例B8の被験者と同じ被験者である。
被験者は75歳の男性で、40歳から50歳頃から頭頂部が薄毛になった。この被験者は、脱毛部位の頭皮に掻痒を伴う紅班、脂漏性鱗屑がみられ、脂漏性脱毛症を合併している男性型脱毛症である。Hamilton-Norwood分類ではVI型に属する。この被験者の父も男性型脱毛症である。この被験者のスクラッチテストの結果は、ハウスダスト2+、ダニ2+、スギ3+、カモガヤ2+、ブタクサ2+でアレルギー性鼻炎の既往がある。この被験者は、ミノキシジルを1年間塗布したが効果はなかった。この被験者は、グリチルレチン酸も2年間使用中であるが効果はない。尚、この被験者は、症例B11の被験者と同じ被験者である。
BNPゲル剤の男性型脱毛症に対する治療効果を表9-1(症例B7~B10)および表9-2(症例B11~B16)に示す。

被験者は39歳の男性で、38歳になって頭頂部がヒリヒリして紅班と鱗屑が出現し頭頂部が薄毛になり、男性型脱毛症になった。Hamilton-Norwood分類ではIIvertex型に属する。この被験者の父方の祖父が男性型脱毛症である。この被験者のスクラッチテストの結果は、ハウスダスト3+、ダニ3+、スギ1+、カモガヤ2+、ブタクサ1+であった。
被験者は45歳の男性で、44歳頃から頭頂部に限局して薄毛になった。この被験者は、脱毛部位頭皮に掻痒を伴う紅班、脂漏性鱗屑がみられ、脂漏性脱毛症を合併している男性型脱毛症である。Hamilton-Norwood分類ではIIvertex型に属する。この被験者の父も、頭頂部に限局した男性型脱毛症である。この被験者のスクラッチテストの結果は、ハウスダスト2+、ダニ3+、カモガヤ1+、ブタクサ1+であった。尚、この被験者は、症例A8の被験者と同じ被験者である。
被験者は42歳の男性で、40歳頃から頭頂部に限局して薄毛になった。この被験者は、脱毛部位頭皮に軽度の紅班と鱗屑がみられる。Hamilton-Norwood分類ではV型に属する。この被験者の父と母方の祖父が男性型脱毛症である。この被験者のスクラッチテストは行なっていない。
被験者は65歳の男性で30代から40代にかけて前頭部と角額部の生え際が後退して薄毛になった。父親も男性型脱毛症である。Hamilton-Norwood分類ではVI型に属する。この被験者のスクラッチテストの結果は、ハウスダスト2+、ダニ2+、スギ1+、カモガヤ1+、ブタクサ1+でアトピー性皮膚炎とアレルギー性結膜炎の既往がある。
被験者は75歳の男性で、40歳から50歳頃から頭頂部が薄毛になった。この被験者は、脱毛部位の頭皮に掻痒を伴う紅班、脂漏性鱗屑がみられ、脂漏性脱毛症を合併している男性型脱毛症である。Hamilton-Norwood分類ではVI型に属する。この被験者の父も男性型脱毛症である。この被験者のスクラッチテストの結果は、ハウスダスト2+、ダニ3+、カモガヤ1+、ブタクサ1+であった。この被験者は、ミノキシジルを1年間塗布したが効果はなかった。この被験者は、グリチルレチン酸も2年間使用中であるが効果はないという。尚、この被験者は、症例A9の被験者と同じ被験者である。
被験者は62歳の男性で、50歳頃から頭頂部が薄毛になり、脱毛部位の頭皮に、掻痒を伴う粃糠様鱗屑と紅班がみられる。この被験者は批糠性脱毛症の合併している男性型脱毛症である。Hamilton-Norwood分類ではIII vertex型に属する。この被験者の父と弟も、男性型脱毛症である。この被験者のスクラッチテストの結果は、ハウスダスト2+、ダニ3+、スギ2+、カモガヤ1+、ブタクサ2+であり、アトピー性皮膚炎と気管支喘息に罹患している。弟がアトピー性皮膚炎、子供はアレルギー性鼻炎の既往がある。

被験者は44歳の男性で、30歳代後半からM型の男性型脱毛症になった。Hamilton-Norwood分類ではIII型に属する、いわゆるM型の脱毛症例である。この被験者の父も男性型脱毛症である。
被験者は46歳の男性で、30歳代後半から前頭部が薄毛になり、40歳を過ぎてから頭頂部も薄毛になった。この被験者は、Hamilton-Norwood分類ではV型に属する、この被験者の父と母方の祖父も男性型脱毛症である。
CNP軟膏剤の男性型脱毛症に対する治療効果を表10(症例C16~C17)に示す。

被験者は56歳の男性であり、40歳代から頭頂部から前頭部にかけて薄毛で軟毛になっている、男性型方脱毛症である。この被験者は、Hamilton-Norwood分類ではVa型に属する、いわゆるM型の脱毛部位とO型の脱毛部位をともに有する症例である。この被験者は、以前、1%ミノキシジルを何年も塗布したが効果がなく、最近では赤くなり掻痒も伴うようになったので使用をやめたという。この被験者の場合、脱毛部位の頭皮に紅班、鱗屑などの炎症症状は出ずに薄毛になったという。この被験者は、父、父方の祖父が男性型脱毛症である。この被験者のスクラッチテストの結果は、ハウスダスト-、ダニ1+、スギ-、カモガヤ-、ブタクサ-であった。
被験者は59歳の男性であり、頭頂部から前頭部にかけて薄毛になっている、男性型脱毛症である。この被験者は、Hamilton-Norwood分類ではVII型に属する、いわゆるM型の脱毛部位とO型の脱毛部位をともに有する症例である。この被験者の場合、脱毛部位の頭皮に紅班、鱗屑、掻爬痕を伴い、掻痒感が強い。この被験者の父、祖父も男性型脱毛症である。この被験者のスクラッチテストの結果は、ハウスダスト2+、ダニ3+、スギ-、カモガヤ2+、ブタクサ2+であった。この被験者は、以前、ステロイドを処方されて7ヶ月外用を継続したが、わずか1時間くらいでまた掻痒感が再燃して炎症がおさまらず、改善しなかった。
CNPゲル剤の男性型脱毛症に対する治療効果を表10-2(症例C24、C37~C39)に示す。
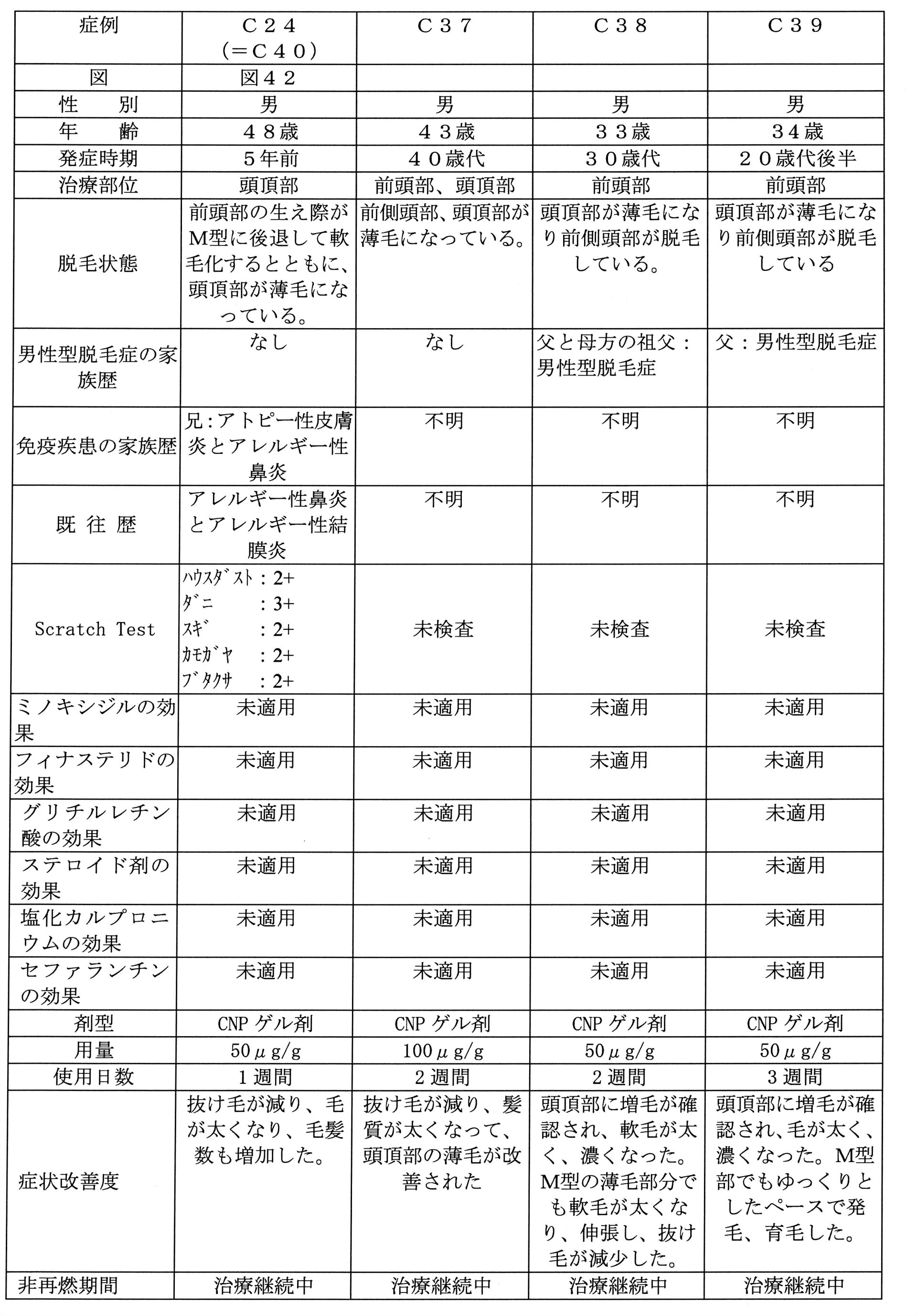
被験者は48歳の男性で、男性型脱毛症である。この被験者は、5年前から前頭部の生え際がM型に後退して軟毛化するとともに、頭頂部が薄毛になった。Hamilton-Norwood分類ではIII vertex型に属する。この被験者に薄毛の家族はいない。
被験者は43歳の男性で、40歳代になってから前側頭部、頭頂部が薄毛になっている、男性型方脱毛症である。この被験者は、Hamilton-Norwood分類ではV型に属する、いわゆるM型の脱毛部位とO型の脱毛部位をともに有する症例である。
被験者は33歳の男性で、20歳代後半から、髪質が縮毛で細くなってきて、30歳代になってからは男性型脱毛症になった。Hamilton-Norwood分類ではIII vertex型に属し、頭頂部が薄毛になり前側頭部が脱毛している、いわゆるM型脱毛症が見られる。この被験者の父、母方の祖父も男性型脱毛症である。
被験者は34歳の男性で、20歳代後半から、薄毛になり、男性型脱毛症になった。Hamilton-Norwood分類ではV型に属し、頭頂部が薄毛になり前側頭部が脱毛している、いわゆるM型脱毛症が見られる。この被験者の父も男性型脱毛症である。この被験者は、1%ミノキシジル溶液を1年間塗布したが効果はなかった。また、この被験者は、ビオチンと漢方薬を内服したが効果がなかった。
この被験者の前頭部に50μg/gのCNPゲル剤を1日2回で3週間塗布したところ、頭頂部に増毛が確認され、毛が太く、濃くなった。M型部でもゆっくりとしたペースで発毛、育毛が観察された。
CNP:ベタメタゾン:ゲンタマイシン合剤の男性型脱毛症に対する治療効果を表10-3(症例C25)に示す。

被験者は75歳の男性で、男性型脱毛症である。この被験者は、5年前から前頭部の生え際がM型に後退し、頭頂部が薄毛になり始めた。また、この被験者は、半年前からは鱗屑、紅班、掻痒を伴っており、批糠性脱毛症を合併している。この被験者は、Hamilton-Norwood分類ではVI型に属する、いわゆるM型脱毛部位とO型脱毛部位をともに有する症例である。
CNP:クロベタゾール合剤の男性型脱毛症に対する治療効果を表10-4(症例C26)に示す。

被験者は61歳の男性で、男性型脱毛症である。この被験者は、前頭部および頭頂部が白髪の混じる薄毛になっており、かゆみと鱗屑を伴っている、批糠性脱毛症を合併している症例である。この被験者の父と父方の祖父、母方の祖父も男性型脱毛症である。この被験者は、気管支喘息を罹患している。この被験者のスクラッチテストの試験結果は、この被験者は、Hamilton-Norwood分類ではIVa型に属する、いわゆるM型脱毛部位とO型脱毛部位をともに有する症例である。この被験者の前頭部および頭頂部にクロベタゾールプロピオン酸エステルを0.05%含有する「デルモベートスカルプローション0.05%(Dermovate Dcalp Lotion 0.05%)」(グラクソ・スミスクライン株式会社)とモメタゾンフランカルボン酸エステルを0.1%含有する「フルメタローション(Fulmeta)」(塩野義製薬株式会社)を9ヶ月間塗布したが、効果は全くみられず、かえって毛髪が薄くなった。
CNP:塩化カルプロニウム合剤の男性型脱毛症に対する治療効果を表10-5(症例C27)に示す。
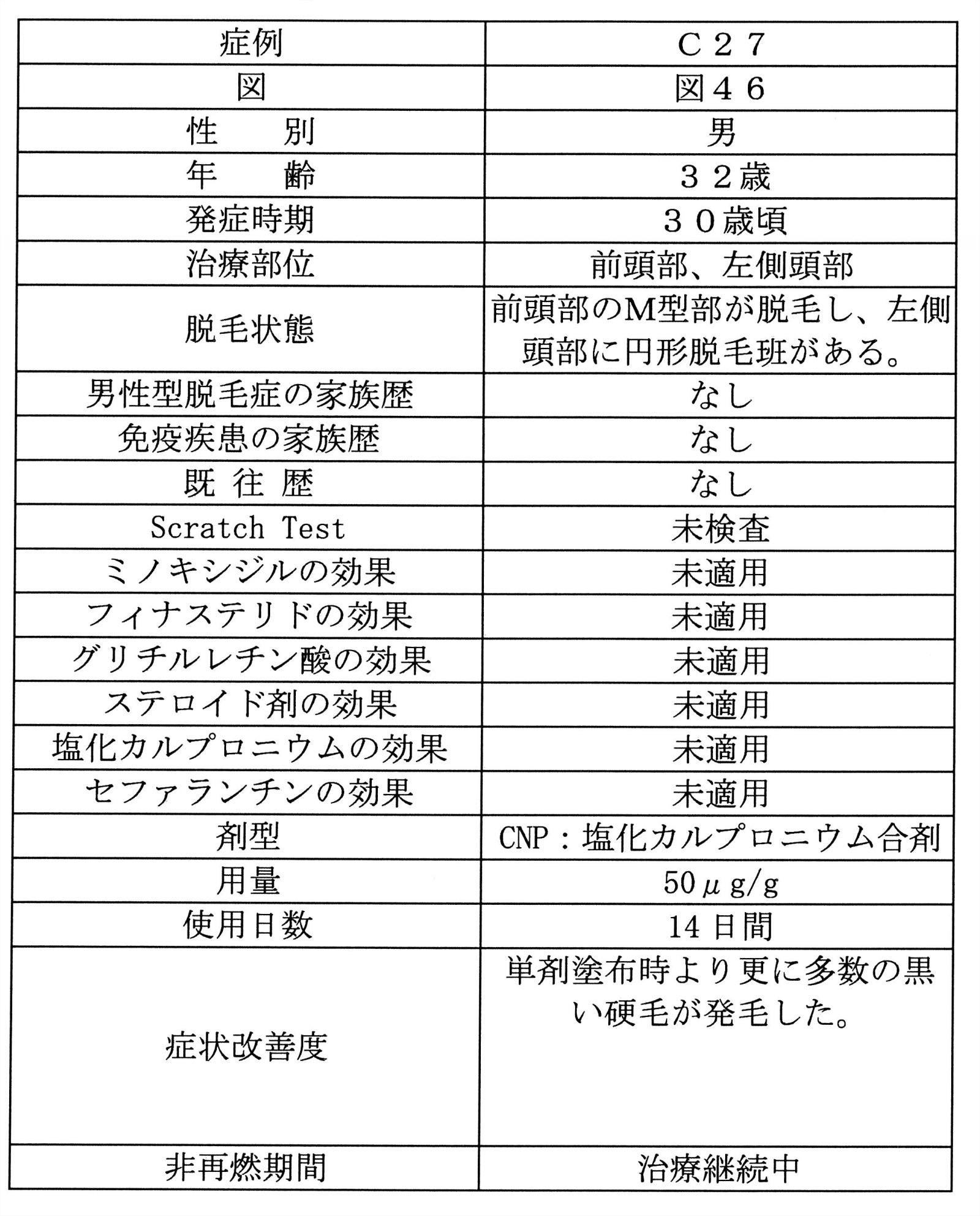
被験者は32歳の男性で、男性型脱毛症である。この被験者は、30歳になって急に前頭部のM型の生え際が薄毛になって後退した。また、来院の6週間前に左側頭部に単発性の円形脱毛症も発症した。この被験者に脱毛症の家族はいない。この被験者は、Hamilton-Norwood分類ではIII型に属する、いわゆるM型の男性型脱毛症である。
CNPゲル剤の塗布を2週間で終了し、その翌日からCNP:塩化カルプロニウム合剤を1日2回塗布したところ、1週間で単剤塗布時より更に多数の黒い硬毛が発毛した。
CNPゲル剤とミノキシジルの重層塗布の男性型脱毛症に対する治療効果を表10-6(症例C40)に示す。

症例C40は、C24と同じ被験者であり、男性型脱毛症の症例である。この症例の詳細は、症例C24の症例として記載したとおりである。
BNPゲル剤とミノキシジルの重層塗布の男性型脱毛症に対する治療効果を表10-7(症例B29)に示す。

被験者は52歳の男性で、Hamilton-Norwood分類ではIV型に属する男性型脱毛症である。この被験者は、23歳頃から前頭部が薄毛になり、現在は、頭頂部も薄毛になっている。この被験者に脱毛症の家族はいない。この被験者は、半夏厚朴湯内服で効果はなかった。
症例C32は、男性型脱毛症と脂漏性脱毛症の合併症例であり、症例A9、B11、B22と同じ症例である。
ANPゲル剤の分娩後脱毛症に対する治療効果を表10-8(症例A10)に示す

この被験者は45歳の女性であり、出産を契機に頭頂部が薄毛になった。
この被験者の頭頂部に100μg/gのANPゲル剤を1日2回で3週間塗布したところ、抜け毛は減らないばかりか頭頂部の脱毛範囲が拡大してしまった。
BNPゲル剤の分娩後脱毛症に対する治療効果を表10-9(症例B17)に示す

症例B17は、症例A10と同じ被験者である。
ANPゲル剤の塗布が終了してから6ヶ月後に、頭頂部に50μg/gのBNPゲル剤を1日3回~4回で3週間塗布したところ、硬毛が増毛して、抜け毛が減少し、薄毛が気にならない程度まで回復した(図47)。
CNPゲル剤の分娩後脱毛症に対する治療効果を表11-1(症例C18)に示す。

被験者は27歳の女性であり、分娩後脱毛症の患者である。アトピー性皮膚炎の既往があり、アトピー素因のある症例である。この被験者の母は、アレルギー性鼻炎を患っており、この被験者の母も頭頂部が薄い女性型脱毛症である。スクラッチテストの結果は、ハウスダスト3+、ダニ3+、スギ2+、カモガヤ2+、ブタクサ2+であった。この被験者は、7月前の出産を契機に急に髪が抜けてしまった。この被験者は、頭頂部から前頭部にかけて薄毛が目立つ。この被験者は、ステロイドと塩化カルプロニウムを5ヶ月間塗布し続けたが、抜け毛が多いままであり、頭頂部の薄毛は改善されなかった。
BNPゲル剤の女性型脱毛症に対する治療効果を表11-2(症例B18~B20、B27)に示す。

被験者は56歳の女性であり、女性型脱毛症の患者である。この被験者は、切れ毛と抜け毛が多く、正中線を中心としたびまん性の脱毛が認められた。この被験者の父、祖父、兄は男性型脱毛症である。
被験者は59歳の女性であり、女性型脱毛症の患者である。この被験者は50代になって前頭部の分け目部分の薄毛が目立つようになった。
被験者は50歳の女性であり、女性型脱毛症の患者である。この被験者は、頭頂部から前頭部にかけて数年前から薄毛になって、分け目が拡大してきた。この被験者の母も女性型脱毛症であり、父は男性型脱毛症である。
被験者は66歳の女性であり、65歳から薄毛になった。頭皮の脂漏性鱗屑が目立つ脂漏性脱毛症を合併した女性型脱毛症である。この被験者は、頭頂部から前頭部、左M型部にかけて薄毛でかなり地肌が透けてみえている。この被験者は、抜け毛が非常に多く、触っただけで直ぐにぬける状態であった。この被験者の父および兄が男性型脱毛症である。
CNPゲル剤の女性型脱毛症に対する治療効果を表12(症例C19、C28およびC29)に示す。

被験者は56歳の女性であり、女性型脱毛症の患者である。アトピー性皮膚炎の既往があり、この被験者の母もアレルギー性鼻炎を患っている、アトピー素因のある症例である。この被験者の父は男性型脱毛症であり、この被験者の母は女性型脱毛症である。スクラッチテストの結果は、ハウスダスト2+、ダニ2+、スギ1+、カモガヤ1+、ブタクサ1+であった。この被験者は、10年前から頭頂部が薄毛になってきている。この被験者は、ステロイドと塩化カルプロニウムの外用では効果がみられなかった。
被験者は62歳の女性であり、女性型脱毛症の患者である。この被験者は、2011年3月11日の東日本大震災後の4月頃から頭皮がかさついてきて前頭部から頭頂部にかけて薄毛になった。この被験者の父は、35歳くらいから男性型脱毛症のため全頭脱毛状態になっている。
被験者は60歳の女性であり、女性型脱毛症の患者である。この被験者は、1年前から鱗屑と掻痒が出現し、前頭部の生え際が薄毛になった。
ANPゲル剤の脂漏性脱毛症に対する治療効果を表13(症例A11、A12)に示す。
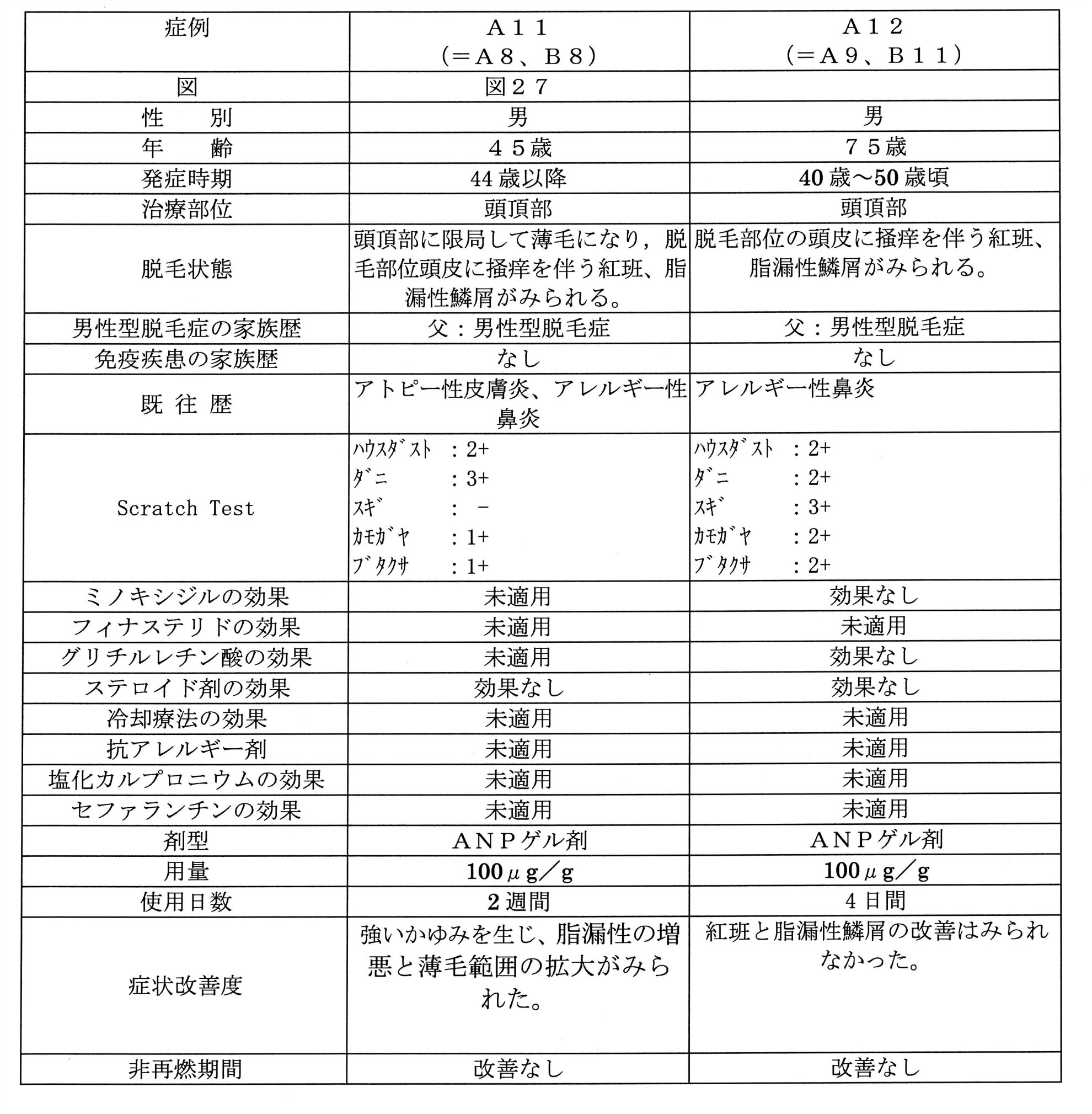
症例A11は、男性型脱毛症と脂漏性脱毛症の合併症例であり、症例A8、B8と同じ症例である。この症例は、その詳細を症例A8、B8の症例として記載したとおりであり、頭頂部の脱毛部位全体に100μg/gのANPゲル剤を朝と晩2回、塗布したところ、2日目には強いかゆみが出て、抜け毛も増えて、脱毛範囲も拡大し、頭皮の脂漏性の増悪と紅班が出現し発毛は観察されなかった。
症例A12は、男性型脱毛症と脂漏性脱毛症の合併症例であり、症例A9、B11と同じ症例である。この症例は、その詳細を症例A9、B11の症例として記載したとおりであり、頭頂部の脱毛部位に100μg/gのANPゲル剤を朝と晩の2回、4日間塗布したが、紅班と脂漏性鱗屑の改善はみられず、脱毛症の改善効果もみられなかった。
BNPゲル剤の脂漏性脱毛症に対する治療効果を表14(症例B21、B22)に示す。

症例B21は、男性型脱毛症と脂漏性脱毛症の合併症例であり、症例A8、B8と同じ症例である。この症例は、その詳細を症例A8、B8の症例として記載したとおりである。
症例B22は、男性型脱毛症と脂漏性脱毛症の合併症例であり、症例A9、B11と同じ症例である。この症例は、その詳細を症例A9、B11の症例として記載したとおりである。
ANPゲル剤の批糠性脱毛症に対する治療効果を表15(症例A13)に示す。

症例A13は、円形脱毛症と批糠性脱毛症の合併症例であり、症例A6、C3、C4、C30と同じ症例である。ただし、CNP軟膏剤は頭頂部に塗布した。この症例は、その詳細を症例A6、C3、C4の症例として記載したとおりでああり、100μg/gのANPゲル剤を2週間塗布しても効果はなく、かさかさした鱗屑が増加して掻痒があり、脱毛範囲がむしろ拡大してしまった。
ANP軟膏剤の批糠性脱毛症に対する治療効果を表15(症例A14)に示す。
症例A14
症例A14は、円形脱毛症と批糠性脱毛症の合併症例であり、症例A1、C5、と同じ症例である。ただし、CNP軟膏剤は2週間の休薬期間をおいた後に塗布した。この症例は、その詳細を症例A1、C5の症例として記載したとおりであり、100μg/gのANPゲル剤を1日2回3週間塗布したところ、軟毛の発毛がみられたが、頭皮の紅斑と批糠性落屑は軽快せず、掻痒もあった。
BNPゲル剤の批糠性脱毛症に対する治療効果を表16(症例B23、B28)に示す。

被験者は81歳の男性であり、3年前から前頭部から頭頂部にかけて薄毛になった。頭皮には粃糠性鱗屑がみられる、老人性脱毛症と批糠性脱毛症の合併症例である。
被験者は59歳の男性であり、批糠性脱毛症である。この被験者は、前頭部から頭頂部にかけてほとんど毛がないくらいの薄毛状態である。2年前から薄毛になり、1年半の間、0.05g/mlのミノキシジルを含有するリアップX5(商標)を1日2回塗布したが、フケがひどくなって、痒みを生じ、4ヶ月前から抜け毛と薄毛が急激に増悪した。この被験者は、洗髪時に、頭皮の鱗屑に髪の毛が大量に付着して抜ける状態であった。
CNPゲル剤の批糠性脱毛症に対する治療効果を表17(症例C30、C31)に示す。

症例C30は、円形脱毛症と批糠性脱毛症の合併症例であり、症例A6、C3、C4、A13と同じ症例である。ただし、CNP軟膏剤は右前頭部に塗布した。この症例は、その詳細を症例A6、C3、C4の症例として記載したとおりであり、100μg/gのCNPゲル剤の1日2回3週間の塗布によって塗布中止後も順調に回復し、塗布中止から8ヶ月経過後も塗布部位に再燃はみられていない。
被験者は42歳の男性であり、批糠性脱毛症の患者である。30歳代後半から前頭部と頭頂部が薄毛になった。2年前から抗真菌剤であるケトコナゾールを2%含有する「外用ニトラゼンクリーム2%(Nitrazen Cream 2%)」(岩城製薬株式会社)および1.2mg/gの合成副腎皮質ホルモンであるベタメタゾン吉草酸エステルと1mg/gの抗生物質であるゲンタマイシンとを含有する「ベトノバールGクリーム(Betnoval G Ointment Cream)」(佐藤製薬株式会社)を塗り続けてきたが全く効果はなかったのみならず、1年前からはフケが厚く付着し、薄毛もさらに悪化した。
そこで、この被験者の前頭部と頭頂部に100μg/gのCNPゲル剤を1日2回で2週間塗布したところ、厚く固着した鱗屑がかなり消失し、頭頂部では増毛し始めた(図52)。
CNP軟膏剤の批糠性脱毛症に対する治療効果を表18(症例C33)に示す。

症例C33は、円形脱毛症と批糠性脱毛症の合併症例であり、症例A6、C3、C4、A13、C30と同じ症例である。ただし、CNP軟膏剤は右前頭部に塗布した。この症例は、その詳細を症例A6、C3、C4の症例として記載したとおりであり、100μg/gのCNP軟膏剤の1日2回2週間塗布することにより、はっきりとした発毛がみとめられ、頭皮の紅斑、鱗屑も消失した。
ANPゲル剤の老人性脱毛症に対する治療効果を表19(症例A15)に示す。

被験者は74歳の男性であり、フケがあり、抜け毛が多く、頭部全体が薄毛になっており、白髪が目立つ、老人性脱毛症である。また、この被験者は、頭皮に強い痒みがあり、フケが多く、抜け毛も多い。
BNPゲル剤の老人性脱毛症に対する治療効果を表20(B24)に示す。

症例B24は、老人性脱毛症と批糠性脱毛症の合併症例であり、症例B23と同じ症例である。そのため、この症例は、その詳細を症例B23として記載したとおりである。
CNPゲル剤の老人性脱毛症に対する治療効果を表21(症例C34)に示す。

被験者は70歳の女性であり、68歳から頭頂部が薄毛になった。被験者によれば、薄毛となった頭頂部の皮膚が萎縮していて触れないくらい痛いという。そこで、50μg/gの濃度のCNPゲル剤を1日2回で3日間塗布したところ、頭皮の痛みが緩和し、抜け毛が少なくなった。その後、さらに3日間塗布を継続したところ、頭皮の紅班は消失し、掻痒、痛みも自覚されなくなって増毛が認められた。
BNPゲル剤の癌化学療法剤性脱毛症に対する治療効果を表22(症例B25)に示す。

被験者は54歳の女性である。被験者は悪性リンパ腫と診断され、2011年4月から9月までの期間にR-CHOP療法を6クール受けた。なお、R-CHOP療法とは、複数の化学療法剤を用いたカクテル療法の一種であり、1日目にヒトB細胞表面抗原であるCD20に対するマウス-ヒト・キメラモノクローナル抗体であるリツキシマブの点滴静注を受け、2日目には、合成副腎皮質ホルモン剤であるプレドニゾロンの錠剤の毎食後内服と、微小管重合阻害剤であるビンクリスチンの静注と、DNAとRNAの合成阻害剤であるドキソルビシンの静注と、DNA合成阻害剤のプロドラッグであるシクロフォスファミドの静注を受け、3日目~6日目には、プレドニゾロンの錠剤のみを毎食後内服し、7日目~21日目は休薬期間とする投与スケジュールを1クールとして、この投与サイクルを繰り返す治療法である。被験者は、第1クール中の2週目から髪が抜け始め、第4クールが終了する7月には全部ぬけてしまった。9月に治療が終了してから徐々に髪が生え始めたものの、生えてきたのは真白い白髪であり、左側生え際部分は後退して非常に薄くなってしまった。
BNPゲル剤の癌化学療法剤性脱毛症に対する治療効果を表23(症例C35)に示す。

被験者は47歳の女性である。被験者は2009年11月に子宮体部癌の切除手術を受けた後、癌化学療法剤であるシスプラチンによる治療を6クール受け、2010年3月に癌化学療法を終了した。被験者はシスプラチンによる治療に伴って全頭脱毛になったのち、シスプラチンによる治療が終了後ほぼ1年経過した2011年5月頃から細くて柔らかい短い毛が生えてきたものの前頭部から頭頂部にかけては薄毛の状態にまでしか回復しなかった。これに対し被験者は、塩化カルプロニウムを6ヶ月間塗布したが、効果はみられなかった。
上記試験例から明らかなとおり、本発明の脱毛症治療剤による脱毛の回復率は非常に高く、その発毛促進効果発現までの期間は短かった。本発明の脱毛症治療剤を1週間から2週間塗布することにより、発毛が確認できる場合がほとんどであり、3週目には明らかな発毛がみられた。また、本発明の治療剤は、白髪を黒髪に回復させ、批糠性脱毛症患者のフケを減少させ、脂漏性脱毛症患者の脂漏性頭皮を改善した。
Claims (28)
- C型ナトリウム利尿ペプチド(CNP)またはB型ナトリウム利尿ペプチド(BNP)を有効成分として含有する脱毛症治療剤。
- 円形脱毛症、男性型脱毛症、脂漏性脱毛症、粃糠性脱毛症、女性型脱毛症、分娩後脱毛症、老人性脱毛症、癌化学療法剤性脱毛症または放射線被爆による脱毛症の治療用の、請求項1に記載の脱毛症治療剤。
- C型ナトリウム利尿ペプチド(CNP)またはB型ナトリウム利尿ペプチド(BNP)が、CNP誘導体またはBNP誘導体である、請求項1に記載の脱毛症治療剤。
- C型ナトリウム利尿ペプチド(CNP)またはB型ナトリウム利尿ペプチド(BNP)が、分子内ジスルフィド結合によって環状構造を形成する、CNPまたはBNPのキメラペプチドであって、
前記CNPが、CNP-22、CNP-53、1~5個の任意のアミノ酸が欠失、置換若しくは付加したCNP-22のアミノ酸配列中の5アミノ酸以上の連続する任意のアミノ酸配列を含むペプチド、または、1~5個の任意のアミノ酸が欠失、置換若しくは付加したCNP-53のアミノ酸配列中の5アミノ酸以上の連続する任意のアミノ酸配列を含むペプチドからなる群より選択されるペプチドであり、
前記BNPが、BNP-26、BNP-32、BNP-45、または、1~5個の任意のアミノ酸が欠失、置換若しくは付加したBNP-26のアミノ酸配列中の5アミノ酸以上の連続する任意のアミノ酸配列を含むペプチド、1~5個の任意のアミノ酸が欠失、置換若しくは付加したBNP-32のアミノ酸配列中の5アミノ酸以上の連続する任意のアミノ酸配列を含むペプチド、1~5個の任意のアミノ酸が欠失、置換若しくは付加したBNP-45のアミノ酸配列中の5アミノ酸以上の連続する任意のアミノ酸配列を含むペプチドからなる群より選択されるペプチドであり、
かつ、CNP活性またはBNP活性を有するキメラペプチド、あるいは、前記のキメラペプチドの誘導体である、請求項1に記載の脱毛症治療剤。 - ベタメタゾン、クロベタゾール、ゲンタマイシン、塩化カルプロニウム、ミノキシジルからなる群から選択される少なく一つの薬剤をさらに含む、請求項1に記載の脱毛症治療剤。
- 白髪の予防剤または治療剤、または、軟毛化の予防剤または治療剤である、請求項1に記載の脱毛症治療剤。
- フケの発生または頭皮の脂漏性を抑制する、請求項1に記載の脱毛症治療剤。
- 男性型脱毛症が、男性の男性型脱毛症または女性の男性型脱毛症である、請求項2に記載の脱毛症治療剤。
- 脱毛部位が前頭部または頭頂部である、請求項8に記載の脱毛症治療剤。
- 脂漏性脱毛症または批糠性脱毛症を合併する、請求項8に記載の脱毛症治療剤。。
- 女性型脱毛症が、脂漏性脱毛症または批糠性脱毛症を合併する女性型脱毛症である、請求項2に記載の脱毛症治療剤。
- 円形脱毛症が、通常型円形脱毛症、全頭脱毛症、汎発性脱毛症または蛇行状脱毛症である、請求項2に記載の脱毛症治療剤。
- 脱毛症が、アレルギー疾患または自己免疫疾患の既往または合併を有する対象の脱毛症である、請求項1に記載の脱毛症治療剤。
- 自己免疫疾患が、慢性円板状エリテマトーデス、限局性強皮症、天疱瘡、類天疱瘡、妊娠性疱疹、線状IgA水疱性皮膚症、後天性表皮水疱症、尋常性白斑、サットン後天性遠心性白斑、自己免疫性の甲状腺疾患、全身性エリテマトーデス、間接リウマチまたは重症筋無力症のいずれかである、請求項13に記載の脱毛症治療剤。
- 脱毛症が、アレルギー疾患の既往もしくは合併を有する対象の脱毛症である、請求項1に記載の脱毛症治療剤。
- 脱毛症が、アトピー性疾患の既往または合併を有する対象の脱毛症である、請求項1に記載の脱毛症治療剤。
- 脱毛症が、紅斑、鱗屑または痂皮を伴う脱毛症である、請求項1に記載の脱毛症治療剤。
- 脱毛症が、アレルギー性皮膚炎またはアレルギー性鼻炎の既往または合併を有する対象の脱毛症である、請求項1に記載の脱毛症治療剤。
- 脱毛症が、ハウスダスト、ダニ、スギ、カモガヤ、ブタクサ、および猫毛からなる群から選択される少なくとも1つのアレルゲンに対するアレルギー反応を示す対象における脱毛症である、請求項1に記載の脱毛症治療剤。
- 脱毛症が、スクラッチテスト、皮内テスト、パッチテスト、特異的IgE抗体試験管内測定法のいずれかのアレルゲン検査において、ハウスダスト、ダニ、スギ、カモガヤ、ブタクサ、および猫毛からなる群から選択される少なくとも1つのアレルゲンに対するアレルギー反応を示す対象における脱毛症である、請求項1に記載の脱毛症治療剤。
- 脱毛症が、ステロイド剤、抗ヒスタミン剤、グリチロン(登録商標)、塩化カルプロニウム、セファランチン、ミノキシジル、フィナステリド、シクロスポリンA、桂枝加竜骨牡蛎湯、半夏厚朴湯、ビオチン、アンスラリン、局所免疫療法、冷却療法、直線偏光近赤外線照射療法、PUVA療法タクロリムスに治療抵抗性を示す脱毛症である、請求項1に記載の脱毛症治療剤。
- 脱毛症が、ステロイド離脱困難状態に至った対象またはステロイド治療剤を使用できない対象の脱毛症である、請求項1に記載の脱毛症治療剤。
- 円形脱毛症が、S1またはB0以上の脱毛症である、請求項2に記載の脱毛症治療剤。
- 1週間以上の塗布で治療効果が得られる、請求項1に記載の脱毛症治療剤。
- 塗布を中止しても1ヶ月以上の期間にわたって再燃しない、請求項1に記載の脱毛症治療剤。
- 剤形が、軟膏剤、ゲル剤、クリーム剤、ローション剤、液剤、ワックス剤、粉末剤、スプレー剤、ゲルスプレー剤、フォーム剤、シャンプー剤、トリートメント剤、頭皮トリートメント剤、または、トニック剤である、請求項1に記載の脱毛症治療剤。
- C型ナトリウム利尿ペプチド(CNP)またはB型ナトリウム利尿ペプチド(BNP)の含有量が、1~1000μg/gである、請求項1に記載の脱毛症治療剤。
- ステロイド剤、抗ヒスタミン剤、血管拡張剤、男性ホルモン活性抑制剤、女性ホルモン剤、抗生物質、抗真菌剤、ペンタデカン、サイトプリン(6-ベンジルアミノプリン)、t-フラバノン、アデノシン、セファランチン、グリチルリチンとメチオニンとグリシンの複合剤であるグリチロン(登録商標)、シクロスポリンA、桂枝加竜骨牡蛎湯(けいしかりゅうこつぼれいとう)、半夏厚朴湯、ビオチン、アンスラリン、タクロリムスおよび三環系抗鬱薬からなる群から選択される少なく一つの薬剤をさらに含む、請求項1に記載の脱毛症治療剤。。
Priority Applications (11)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| EP12736336.4A EP2666475B1 (en) | 2011-01-21 | 2012-01-20 | Therapeutic agent for alopecia |
| DK12736336.4T DK2666475T3 (da) | 2011-01-21 | 2012-01-20 | Terapeutisk middel til skaldethed |
| ES12736336.4T ES2647680T3 (es) | 2011-01-21 | 2012-01-20 | Fármaco terapéutico para la alopecia |
| MX2013008422A MX353295B (es) | 2011-01-21 | 2012-01-20 | Agente para el tratamiento de la alopecia. |
| JP2012549041A JP5261620B2 (ja) | 2011-01-21 | 2012-01-20 | 脱毛症治療剤 |
| KR1020137021710A KR101954869B1 (ko) | 2011-01-21 | 2012-01-20 | 탈모증 치료제 |
| CA2825382A CA2825382C (en) | 2011-01-21 | 2012-01-20 | An agent comprising a natriuretic peptide for the treatment of alopecia |
| BR112013018679-8A BR112013018679B1 (pt) | 2011-01-21 | 2012-01-20 | Agente para o tratamento da alopecia e uso de um peptídeo natriurético do tipo c |
| AU2012207816A AU2012207816B2 (en) | 2011-01-21 | 2012-01-20 | Therapeutic agent for alopecia |
| CN201280013887.7A CN103547282A (zh) | 2011-01-21 | 2012-01-20 | 秃头症治疗剂 |
| AU2017203793A AU2017203793A1 (en) | 2011-01-21 | 2017-06-05 | Therapeutic agent for alopecia |
Applications Claiming Priority (2)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| JP2011-011437 | 2011-01-21 | ||
| JP2011011437 | 2011-01-21 |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| WO2012099258A1 true WO2012099258A1 (ja) | 2012-07-26 |
Family
ID=46515875
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/JP2012/051272 WO2012099258A1 (ja) | 2011-01-21 | 2012-01-20 | 脱毛症治療剤 |
Country Status (14)
| Country | Link |
|---|---|
| US (4) | US20120238498A1 (ja) |
| EP (2) | EP2666475B1 (ja) |
| JP (1) | JP5261620B2 (ja) |
| KR (1) | KR101954869B1 (ja) |
| CN (2) | CN103547282A (ja) |
| AU (2) | AU2012207816B2 (ja) |
| BR (1) | BR112013018679B1 (ja) |
| CA (1) | CA2825382C (ja) |
| DK (1) | DK2666475T3 (ja) |
| ES (1) | ES2647680T3 (ja) |
| HU (1) | HUE035584T2 (ja) |
| MX (1) | MX353295B (ja) |
| TW (2) | TWI619505B (ja) |
| WO (1) | WO2012099258A1 (ja) |
Cited By (4)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2016194855A1 (ja) * | 2015-05-29 | 2016-12-08 | 株式会社イギス | 環状ペプチド並びに該環状ペプチドを含む医薬、外用剤および化粧料 |
| WO2017022728A1 (ja) * | 2015-07-31 | 2017-02-09 | 株式会社イギス | Cnp環状ペプチド並びに該環状ペプチドを含む医薬品、外用剤および化粧料 |
| US9968654B2 (en) | 2009-07-23 | 2018-05-15 | Igisu Co., Ltd. | Method of treatment dermatitis with c-type natriuretic peptide derivatives |
| EP3500592A4 (en) * | 2016-08-18 | 2020-08-12 | National University of Singapore | PEPTIDES WITH VASODILATOR AND / OR DIURETIC FUNCTIONS |
Families Citing this family (14)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| EP2666475B1 (en) | 2011-01-21 | 2017-08-16 | Igisu Co., Ltd. | Therapeutic agent for alopecia |
| KR101833776B1 (ko) * | 2015-04-28 | 2018-03-02 | (주) 메드빌 | 지모와 두릅의 복합 추출물을 함유하는 탈모 방지 및 발모 개선용 조성물 |
| US20170135969A1 (en) | 2015-11-12 | 2017-05-18 | Jds Therapeutics, Llc | Topical arginine-silicate-inositol for wound healing |
| CN105617360B (zh) * | 2015-12-04 | 2018-12-21 | 中国农业大学 | C-型钠肽在制备外用避孕药和精子功能检测试剂中的应用 |
| KR102160565B1 (ko) * | 2016-03-18 | 2020-09-28 | (주)케어젠 | 피나스테라이드와 펩타이드의 결합체 |
| WO2017165452A1 (en) * | 2016-03-21 | 2017-09-28 | Rhode Island Council On Postsecondary Education | pH-SENSITIVE PEPTIDES |
| KR101948238B1 (ko) * | 2016-08-19 | 2019-02-14 | (주)케어젠 | 미녹시딜과 펩타이드의 결합체 |
| WO2018045244A1 (en) | 2016-09-01 | 2018-03-08 | Jds Therapeutics, Llc | Magnesium biotinate compositions and methods of use |
| WO2018049174A1 (en) * | 2016-09-08 | 2018-03-15 | Synergistic Therapeutics, Llc | Topical hair growth formulation |
| CN108424446A (zh) * | 2017-02-13 | 2018-08-21 | 成都贝爱特生物科技有限公司 | 新的重组人心房利钠肽突变体的制备及其应用 |
| EP3760214A4 (en) * | 2018-02-28 | 2021-11-17 | Mother"S Pharmaceutical Co.,Ltd. | COMPOSITION TO PREVENT HAIR LOSS OR STIMULATE HAIR GROWTH |
| CN109011138A (zh) * | 2018-05-07 | 2018-12-18 | 北京全贵医疗科技有限公司 | 基于头部图像的头部理疗方法及装置 |
| WO2020123312A1 (en) | 2018-12-09 | 2020-06-18 | Weinberg Assa | Method to prevent and treat macular degeneration by vasodilators |
| WO2020154304A1 (en) * | 2019-01-24 | 2020-07-30 | Weinberg Assa | Method to prevent and treat alopecia by calcium channel blockers, angiotensin converting enzyme inhibitors, and angiotensin receptor blockers |
Citations (26)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US4804650A (en) | 1986-10-28 | 1989-02-14 | Biotechnology Research Associates, J.V. | Analogs of atrial natriuretic peptides |
| US5047397A (en) | 1988-08-26 | 1991-09-10 | California Biotechnology Inc. | Linear analogs of atrial natriuretic peptides |
| US5114923A (en) | 1988-05-31 | 1992-05-19 | California Biotechnology Inc. | Recombinant techniques for production of novel natriuretic and vasodilator peptides |
| US5204328A (en) | 1990-06-26 | 1993-04-20 | Merck & Co., Inc. | Peptides having atrial natriuretic factor activity |
| JPH05207891A (ja) | 1991-03-08 | 1993-08-20 | Shionogi & Co Ltd | 脳性ナトリウム利尿ペプチドの製造方法 |
| JPH069688A (ja) | 1991-01-31 | 1994-01-18 | Toshiyuki Matsuo | Cnp類似体ペプチド及びその用途 |
| US5583108A (en) | 1993-03-03 | 1996-12-10 | Mayo Foundation For Medical Education And Research | Vasonatrin peptide and analogs thereof |
| US6028055A (en) | 1996-10-22 | 2000-02-22 | Genetech, Inc. | Receptor selective BNP |
| JP2000169387A (ja) | 1998-09-28 | 2000-06-20 | Santen Pharmaceut Co Ltd | ナトリウム利尿ペプチドを有効成分とする涙液分泌促進または角結膜障害治療用点眼剤 |
| JP2000516836A (ja) | 1997-05-23 | 2000-12-19 | バクスター インターナショナル インコーポレイテッド | 腹膜透析溶液への添加剤としての心房性ナトリウム利尿ペプチド(anp) |
| US6818619B2 (en) | 1999-12-17 | 2004-11-16 | Mayo Foundation For Medical Education And Research | Chimeric natriuretic peptides |
| WO2004110489A1 (ja) | 2003-06-13 | 2004-12-23 | Daiichi Asubio Pharma Co., Ltd. | Th1型免疫疾患予防又は治療用医薬組成物 |
| WO2005094889A1 (ja) | 2004-03-31 | 2005-10-13 | Chugai Seiyaku Kabushiki Kaisha | 関節炎症治療剤又は予防剤 |
| WO2005094890A1 (ja) | 2004-03-31 | 2005-10-13 | Kazuwa Nakao | 身長増加用組成物 |
| JP2007070336A (ja) * | 2005-08-12 | 2007-03-22 | Takehito Kono | 育毛物質 |
| JP2007525213A (ja) | 2004-01-27 | 2007-09-06 | コンピュゲン ユーエスエイ,インク. | 新規の脳性ナトリウム利尿ペプチドの変異体及びその利用方法 |
| JP2007525957A (ja) | 2003-06-20 | 2007-09-13 | メイヨ・ファウンデーション・フォー・メディカル・エデュケーション・アンド・リサーチ | 脳性ナトリウム利尿ペプチドのアイソフォーム |
| WO2008032450A1 (fr) | 2006-09-15 | 2008-03-20 | Kyoto University | Agent prophylactique et/ou thérapeutique pour une stéatose hépatique |
| JP2008162987A (ja) | 2006-12-31 | 2008-07-17 | Toshiko Koide | 心房利尿ホルモンファミリー分子を活性物質として含有する組織再生製剤また該製剤をもちいる組織再生方法、および心房利尿ホルモンファミリー分子を活性物質として含有する発毛、増毛、育毛剤および皮膚組織修復改善剤また該製剤を用いる発毛、増毛、育毛促進方法および皮膚組織修復改善方法 |
| JP2008540509A (ja) * | 2005-05-09 | 2008-11-20 | フォーミックス エルティーディー. | 血管作用性キットおよび組成物ならびにその用途 |
| WO2008140125A1 (ja) | 2007-05-10 | 2008-11-20 | National University Corporation Nagoya University | 腹膜線維化抑制用医薬組成物 |
| JP2009013122A (ja) * | 2007-07-06 | 2009-01-22 | Masaru Okura | 育毛剤 |
| JP2010500032A (ja) | 2006-08-08 | 2010-01-07 | メイヨ・ファウンデーション・フォー・メディカル・エデュケーション・アンド・リサーチ | 利尿ポリペプチドおよびナトリウム利尿ポリペプチド |
| JP2010168283A (ja) | 2007-04-24 | 2010-08-05 | Yamaguchi Univ | ナトリウム利尿ペプチドを有効成分とする肝硬変・前癌病変の抑制剤 |
| JP2010539022A (ja) * | 2007-09-11 | 2010-12-16 | モンドバイオテック ラボラトリーズ アクチエンゲゼルシャフト | 治療剤としての、c型ナトリウム利尿ペプチド単独または神経ペプチドafとの組合せの使用 |
| JP2010280696A (ja) * | 2003-02-07 | 2010-12-16 | Teikoku Pharma Usa Inc | 皮膚用薬の対象への投与方法 |
Family Cites Families (19)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| TW382595B (en) * | 1993-10-15 | 2000-02-21 | Merck & Co Inc | Pharmaceutical composition for use in arresting and reversing androgenic alopecia |
| IL142118A0 (en) * | 2001-03-20 | 2002-03-10 | Prochon Biotech Ltd | Method and composition for treatment of skeletal dysplasias |
| WO2004022003A2 (en) | 2002-09-06 | 2004-03-18 | University Of South Florida | Materials and methods for treatment of allergic diseases |
| KR100509446B1 (ko) | 2003-06-19 | 2005-08-22 | 세메스 주식회사 | 반도체 제조 공정에서 사용되는 약액 공급 장치 |
| GB2403533A (en) * | 2003-06-30 | 2005-01-05 | Orion Corp | Atrial natriuretic peptide and brain natriuretic peptide and assays and uses thereof |
| WO2005072055A2 (en) | 2004-01-27 | 2005-08-11 | Compugen Usa, Inc. | Novel brain natriuretic peptide variants and methods of use thereof |
| TW200616660A (en) | 2004-08-11 | 2006-06-01 | Alza Corp | Apparatus and method for transdermal delivery of natriuretic peptides |
| EP1810716A1 (de) | 2005-12-23 | 2007-07-25 | Deutsches Zentrum für Luft- und Raumfahrt e.V. | Verfahren zur Bräunung der Haut |
| US7196223B2 (en) * | 2005-05-03 | 2007-03-27 | Solutia, Inc. | Higher alcohols for solvents in amine production |
| KR100842392B1 (ko) | 2006-10-10 | 2008-07-01 | 주식회사 일진글로벌 | 토크를 측정할 수 있는 구동휠시스템 |
| JP2008140125A (ja) | 2006-12-01 | 2008-06-19 | Rakuten Inc | サービス予約システム、予約登録装置、参加者募集方法及び参加者募集処理プログラム |
| US20120034183A1 (en) | 2006-12-19 | 2012-02-09 | Michael Cohen | Compositions and methods for growing embryonic stem cells |
| JP2010539027A (ja) | 2007-09-11 | 2010-12-16 | モンドバイオテック ラボラトリーズ アクチエンゲゼルシャフト | 治療剤としてのペプチドの使用 |
| AR069409A1 (es) | 2007-11-21 | 2010-01-20 | Biomarin Pharm Inc | Variantes de peptidos natriureticos de tipo c |
| US8455438B2 (en) * | 2008-12-29 | 2013-06-04 | Mayo Foundation For Medical Education And Research | Natriuretic polypeptides for reducing or preventing restenosis |
| US20110014180A1 (en) * | 2009-07-16 | 2011-01-20 | Masafumi Koide | Preparations for tissue restoration containing atrial diuretic hormone and family molecules as active ingredients; method of restoring tissue using the preparation; agents for growing, restoring, promoting growth of hair and agents for promoting restoration of skin tissue and cardiac muscle tissue containing atrial diuretic hormone family molecules as active ingredients; method of growing, restoring, promoting growth of hair by using the agents; and method of promoting restoration of skin tissue and cardiac muscle tissue |
| CN105999230B (zh) * | 2009-07-23 | 2022-06-24 | Igisu株式会社 | 皮肤外用剂组合物 |
| US20130045921A1 (en) * | 2009-08-27 | 2013-02-21 | Igisu Company, Ltd | Therapeutic agent for rhinitis |
| EP2666475B1 (en) | 2011-01-21 | 2017-08-16 | Igisu Co., Ltd. | Therapeutic agent for alopecia |
-
2012
- 2012-01-20 EP EP12736336.4A patent/EP2666475B1/en active Active
- 2012-01-20 AU AU2012207816A patent/AU2012207816B2/en active Active
- 2012-01-20 CN CN201280013887.7A patent/CN103547282A/zh active Pending
- 2012-01-20 WO PCT/JP2012/051272 patent/WO2012099258A1/ja active Application Filing
- 2012-01-20 DK DK12736336.4T patent/DK2666475T3/da active
- 2012-01-20 EP EP17184915.1A patent/EP3269382A1/en not_active Withdrawn
- 2012-01-20 HU HUE12736336A patent/HUE035584T2/en unknown
- 2012-01-20 KR KR1020137021710A patent/KR101954869B1/ko active IP Right Grant
- 2012-01-20 BR BR112013018679-8A patent/BR112013018679B1/pt active IP Right Grant
- 2012-01-20 CN CN201910952287.0A patent/CN110801514A/zh active Pending
- 2012-01-20 MX MX2013008422A patent/MX353295B/es active IP Right Grant
- 2012-01-20 CA CA2825382A patent/CA2825382C/en active Active
- 2012-01-20 JP JP2012549041A patent/JP5261620B2/ja not_active Expired - Fee Related
- 2012-01-20 ES ES12736336.4T patent/ES2647680T3/es active Active
- 2012-01-21 US US13/355,484 patent/US20120238498A1/en not_active Abandoned
- 2012-01-30 TW TW101102860A patent/TWI619505B/zh active
- 2012-01-30 TW TW106138356A patent/TW201811360A/zh unknown
-
2014
- 2014-04-17 US US14/254,938 patent/US9480728B2/en active Active
-
2016
- 2016-09-20 US US15/270,350 patent/US9808511B2/en active Active
-
2017
- 2017-06-05 AU AU2017203793A patent/AU2017203793A1/en not_active Abandoned
- 2017-10-06 US US15/726,519 patent/US11571464B2/en active Active
Patent Citations (26)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US4804650A (en) | 1986-10-28 | 1989-02-14 | Biotechnology Research Associates, J.V. | Analogs of atrial natriuretic peptides |
| US5114923A (en) | 1988-05-31 | 1992-05-19 | California Biotechnology Inc. | Recombinant techniques for production of novel natriuretic and vasodilator peptides |
| US5047397A (en) | 1988-08-26 | 1991-09-10 | California Biotechnology Inc. | Linear analogs of atrial natriuretic peptides |
| US5204328A (en) | 1990-06-26 | 1993-04-20 | Merck & Co., Inc. | Peptides having atrial natriuretic factor activity |
| JPH069688A (ja) | 1991-01-31 | 1994-01-18 | Toshiyuki Matsuo | Cnp類似体ペプチド及びその用途 |
| JPH05207891A (ja) | 1991-03-08 | 1993-08-20 | Shionogi & Co Ltd | 脳性ナトリウム利尿ペプチドの製造方法 |
| US5583108A (en) | 1993-03-03 | 1996-12-10 | Mayo Foundation For Medical Education And Research | Vasonatrin peptide and analogs thereof |
| US6028055A (en) | 1996-10-22 | 2000-02-22 | Genetech, Inc. | Receptor selective BNP |
| JP2000516836A (ja) | 1997-05-23 | 2000-12-19 | バクスター インターナショナル インコーポレイテッド | 腹膜透析溶液への添加剤としての心房性ナトリウム利尿ペプチド(anp) |
| JP2000169387A (ja) | 1998-09-28 | 2000-06-20 | Santen Pharmaceut Co Ltd | ナトリウム利尿ペプチドを有効成分とする涙液分泌促進または角結膜障害治療用点眼剤 |
| US6818619B2 (en) | 1999-12-17 | 2004-11-16 | Mayo Foundation For Medical Education And Research | Chimeric natriuretic peptides |
| JP2010280696A (ja) * | 2003-02-07 | 2010-12-16 | Teikoku Pharma Usa Inc | 皮膚用薬の対象への投与方法 |
| WO2004110489A1 (ja) | 2003-06-13 | 2004-12-23 | Daiichi Asubio Pharma Co., Ltd. | Th1型免疫疾患予防又は治療用医薬組成物 |
| JP2007525957A (ja) | 2003-06-20 | 2007-09-13 | メイヨ・ファウンデーション・フォー・メディカル・エデュケーション・アンド・リサーチ | 脳性ナトリウム利尿ペプチドのアイソフォーム |
| JP2007525213A (ja) | 2004-01-27 | 2007-09-06 | コンピュゲン ユーエスエイ,インク. | 新規の脳性ナトリウム利尿ペプチドの変異体及びその利用方法 |
| WO2005094889A1 (ja) | 2004-03-31 | 2005-10-13 | Chugai Seiyaku Kabushiki Kaisha | 関節炎症治療剤又は予防剤 |
| WO2005094890A1 (ja) | 2004-03-31 | 2005-10-13 | Kazuwa Nakao | 身長増加用組成物 |
| JP2008540509A (ja) * | 2005-05-09 | 2008-11-20 | フォーミックス エルティーディー. | 血管作用性キットおよび組成物ならびにその用途 |
| JP2007070336A (ja) * | 2005-08-12 | 2007-03-22 | Takehito Kono | 育毛物質 |
| JP2010500032A (ja) | 2006-08-08 | 2010-01-07 | メイヨ・ファウンデーション・フォー・メディカル・エデュケーション・アンド・リサーチ | 利尿ポリペプチドおよびナトリウム利尿ポリペプチド |
| WO2008032450A1 (fr) | 2006-09-15 | 2008-03-20 | Kyoto University | Agent prophylactique et/ou thérapeutique pour une stéatose hépatique |
| JP2008162987A (ja) | 2006-12-31 | 2008-07-17 | Toshiko Koide | 心房利尿ホルモンファミリー分子を活性物質として含有する組織再生製剤また該製剤をもちいる組織再生方法、および心房利尿ホルモンファミリー分子を活性物質として含有する発毛、増毛、育毛剤および皮膚組織修復改善剤また該製剤を用いる発毛、増毛、育毛促進方法および皮膚組織修復改善方法 |
| JP2010168283A (ja) | 2007-04-24 | 2010-08-05 | Yamaguchi Univ | ナトリウム利尿ペプチドを有効成分とする肝硬変・前癌病変の抑制剤 |
| WO2008140125A1 (ja) | 2007-05-10 | 2008-11-20 | National University Corporation Nagoya University | 腹膜線維化抑制用医薬組成物 |
| JP2009013122A (ja) * | 2007-07-06 | 2009-01-22 | Masaru Okura | 育毛剤 |
| JP2010539022A (ja) * | 2007-09-11 | 2010-12-16 | モンドバイオテック ラボラトリーズ アクチエンゲゼルシャフト | 治療剤としての、c型ナトリウム利尿ペプチド単独または神経ペプチドafとの組合せの使用 |
Non-Patent Citations (29)
Cited By (10)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US9968654B2 (en) | 2009-07-23 | 2018-05-15 | Igisu Co., Ltd. | Method of treatment dermatitis with c-type natriuretic peptide derivatives |
| WO2016194855A1 (ja) * | 2015-05-29 | 2016-12-08 | 株式会社イギス | 環状ペプチド並びに該環状ペプチドを含む医薬、外用剤および化粧料 |
| JPWO2016194855A1 (ja) * | 2015-05-29 | 2018-06-07 | 株式会社 イギス | 環状ペプチド並びに該環状ペプチドを含む医薬、外用剤および化粧料 |
| JP2021073234A (ja) * | 2015-05-29 | 2021-05-13 | 株式会社 イギス | 環状ペプチド並びに該環状ペプチドを含む医薬、外用剤および化粧料 |
| EP4014987A2 (en) | 2015-05-29 | 2022-06-22 | Igisu Co., Ltd. | Cyclic peptide, and medicine, external preparation and cosmetic each containing said cyclic peptide |
| WO2017022728A1 (ja) * | 2015-07-31 | 2017-02-09 | 株式会社イギス | Cnp環状ペプチド並びに該環状ペプチドを含む医薬品、外用剤および化粧料 |
| JPWO2017022728A1 (ja) * | 2015-07-31 | 2018-06-21 | 株式会社 イギス | Cnp環状ペプチド並びに該環状ペプチドを含む医薬品、外用剤および化粧料 |
| JP7253220B2 (ja) | 2015-07-31 | 2023-04-06 | 株式会社 イギス | Cnp環状ペプチド並びに該環状ペプチドを含む医薬品、外用剤および化粧料 |
| EP3500592A4 (en) * | 2016-08-18 | 2020-08-12 | National University of Singapore | PEPTIDES WITH VASODILATOR AND / OR DIURETIC FUNCTIONS |
| US11312758B2 (en) | 2016-08-18 | 2022-04-26 | National University Of Singapore | Peptides with vasodilatory and/or diuretic functions |
Also Published As
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| JP5261620B2 (ja) | 脱毛症治療剤 | |
| JP6337071B2 (ja) | 皮膚外用剤組成物 |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application |
Ref document number: 12736336 Country of ref document: EP Kind code of ref document: A1 |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2012549041 Country of ref document: JP |
|
| WWE | Wipo information: entry into national phase |
Ref document number: MX/A/2013/008422 Country of ref document: MX |
|
| ENP | Entry into the national phase |
Ref document number: 2825382 Country of ref document: CA |
|
| NENP | Non-entry into the national phase |
Ref country code: DE |
|
| REEP | Request for entry into the european phase |
Ref document number: 2012736336 Country of ref document: EP |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2012736336 Country of ref document: EP |
|
| ENP | Entry into the national phase |
Ref document number: 20137021710 Country of ref document: KR Kind code of ref document: A |
|
| ENP | Entry into the national phase |
Ref document number: 2012207816 Country of ref document: AU Date of ref document: 20120120 Kind code of ref document: A |
|
| REG | Reference to national code |
Ref country code: BR Ref legal event code: B01A Ref document number: 112013018679 Country of ref document: BR |
|
| ENP | Entry into the national phase |
Ref document number: 112013018679 Country of ref document: BR Kind code of ref document: A2 Effective date: 20130722 |